Download
1 / 60
610 likes | 695 Views
Learn about the role of echocardiography in diagnosing and managing aortic regurgitation, including hemodynamics, LV assessment, and more. Understand the functional anatomy and assessment techniques for AR.

E N D
Aortic Regurgitation 2D and Doppler Assessment Dr.Sohail Abrar Khan MBBS,FCPS (Med), FCPS (Card) Diplomate of American certification Board of Echo Assistant Professor and Consultant Cardiologist Aga Khan University Hospital Karachi
Introduction • Aortic regurgitation is a common and serious health problem • Echo is the most valuable tool in the diagnosis and management of AR • Echo evaluation of AR requires a comprehensive evaluation by an experienced person • Visual and qualitative assessment may be unreliable and misleading
Introductioncont… • Patients are often asymptomatic until AR becomes significant • AR murmur usually not heard until AR severity > mild • Detection of AR may be the first clue that aortic root or aortic valve disease is present
Role of Echo in Assessment AR • 2D and Doppler echocardiography is indispensable in the diagnosis and management of patients with AR • This should be used to assess the severity of AR, the LV response to volume overload (systolic function, ejection fraction [EF] and end-systolic and diastolic dimensions). • Echocardiography may also identify the anatomic cause of AR, which is important for determining the surgical approach
Assessment of Regurgitation 2D Echo CFI AR Hemodynamics ERO/R Vol ERO/RV CW Doppler PW Doppler
Hemodynamics of AR Chronic AR • Progressive ↑ AR • Heart has time to compensate • ↑ LV volume • ↑ dilatation • ↑ Stroke Volume Acute AR • Rapid onset of AR • Insufficient time for heart to compensate • Leads to ↑ LVEDP • Pulmonary edema • Decreased effective forward Stroke vol
Hemodynamics of AR cont… Acute AR Chronic AR Adapted From: Lilly L. Pathophysiology of Heart Disease
Aortic Regurgitation2D Echo • Assess valvular function • Identification of functional anatomy • Assess LV size and function • Evidence of increased LVEDP
2D Echo cont… Assessment of LV • Serial reproducible findings • LV chamber enlargement • LV function assessment • Predictors of preserved LV function after AVR • LVESD < 55 mm • LV EF > 50%
89±3% LVS/BSA <25 81±5% 50±9% LVS/BSA ³25 Survival (%) 34±10% Years Conservative Rx for Severe AR Survival vs Indexed LV Systolic Diameter Dujardin KS: Circ,99 CP993609-9
Aortic Regurgitation2-D and M-Mode Clues of AR • Diastolic fluttering of anterior MV leaflet • Reverse “doming” of anterior MV leaflet • Diastolic flutter of aortic valve Evidence for increased LVEDP • Presystolic (premature) closure of MV • Presystolic (premature) opening of AV
Aortic Regurgitation Functional Anatomy Valvular • Congenital (bicuspid) • Degenerative • Rheumatic • Endocarditis • Cusp rupture
Functional Anatomy cont… Aortic Root Chronic Dilatation • Marfan syndrome • Senile/hypertensive • Chronic aortitis • Idiopathic Annuloaorticectasia • Sinus of valsalva aneurysm Acute Disruption • Dissection • Chest trauma • Endocarditis • Post-procedure
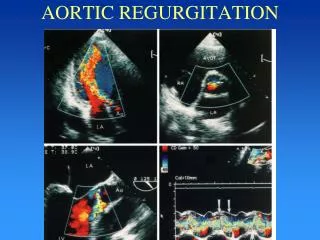
Aortic RegurgitationColor Flow Imaging Jet area ¸ LVOT area Jet width ¸ LVOT width CP993609-12
Color Flow Imaging cont…Jet Width/LVOT Width Perry et al. JACC 1987
Color Flow Imaging cont…Jet area/LVOT area • AR jet area and LVOT area from parasternal short axis view • Correlates best with angiographic severity of AR • Assess AR at the level of the aortic annulus, just below the AV Oh, Seward,Tajik: The Echo Manual
Color Flow Imaging cont…Jet area/LVOT area Grade I < 5% Grade II 5 - 24% Grade III 25 - 59% Grade IV > 60%
Vena Contracta Measure from PLAX (zoom) Use standard color scale No baseline shift Measure width of AR jet at the narrowest point Measure just below flow convergence Vena contracta < 6 mm = severe AR Vena contracta < 3 mm = mild AR
VC Width 5 mm 6 mm7 mm Sn Sp Sn Sp Sn Sp 2 ERO≥0.3 cm 100 73 95 90 84 95 RegVol≥60 ml 96 81 81 94 65 96 Vena Contractacont… Tribouilloy et al: Circulation, 2000
Vena Contracta Optimize the flow convergence zone
Vena Contracta Vena contracta is usually smaller than LVOT jet height Measure width of AR at narrowest point of emitting jet
Aortic RegurgitationCW Doppler Assessment • Density of CW signal reflects Reg Vol • Pressure half-time • Mild AR > 400 msec • Severe AR < 250 msec Oh,Seward, Tajik: The Echo Manual
Align Doppler parallel to flow Move lateral or try a lower rib space
CW Doppler Assessment cont… Pressure Half Time PHT • Mild AR > 400 msec Otto and Pearlman: Textbook of Clinical Echocardiography
CW Doppler Assessment cont… Pressure Half Time PHT Severe AR < 250 msec Otto and Pearlman: Textbook of Clinical Echocardiography
CW Doppler Assessment cont… • AR PHT may be shortened due to other causes of elevated LVEDP i.e LV systolic and diastolic dysfunction and Mitral Regurgitation • It can be increased due to Mitral Stenosis
Aortic RegurgitationPW Doppler Assessment • LV stroke volume • Mitral inflow • Descending thoracic aorta • Abdominal aorta
PW Doppler cont… Mitral Inflow • High LA Pressure & LVEDP • Restrictive mitral inflow • Mitral pattern dependent on compliance of ventricle Oh,Seward, Tajik: The Echo Manual
PW Doppler cont… Premature Cessation of Mitral Flow in Acute Severe AR Pre-op Post-op
PW Doppler cont… CP993609-21
PW Doppler cont… Descending Aorta • Diastolic flow reversal • Retrograde flow TVI Severe AR TVI > 14 cm
PW Doppler cont… Abdominal Aorta • Place PW sample volume in abdominal aorta • Diastolic flow reversal consistent with significant aortic regurgitation Otto and Pearlman: Textbook of Clinical Echocardiography
Indications for Quantitative Doppler • When regurgitation appears moderate or more by CFI/qualitative assessment • Serial assessment • Assess LV size & function • Assess regurgitation • Assist clinician/surgeon • Clinical management • Timing of surgery
Quantitative Doppler Methods Continuity Equation PISA Method CSA TVI
Continuity Equation Stroke volume Valve area Shunt lesions Regurgitant volume Regurgitant fraction
Continuity Equation cont… What goes in (the ventricle) must go out!!
Regurgitant Volume Volume of blood that regurgitates through an incompetent valve with each heart beat
Continuity Equation Calculation TVI A A = X Area TVI Stroke volume CP944143- 6
Continuity Method cont… “What goes in must go out” Measurements required LVOT diameter & TVI MV annulus diameter & TVI Limitation of continuity method Unable to use with multiple regurgitant lesions > mild and shunt lesions
Continuity Method cont… Calculate SVLVOT Measure LVOT diameter Obtain PW Doppler signal in LVOT Trace LVOT TVI SVLVOT = CSALVOT x TVILVOT
Continuity Method cont… Calculate SVMV Measure diameter of mitral annulus Obtain PW Doppler signal at level of mitral annulus Trace MV annulus TVI SVMV = CSAMV x TVIMV
Regurgitant Volume and Fraction SVLVOT = CSALVOT x TVILVOT SVMV = CSAMV x TVIMV RVAR =SVLVOT- SVMV RFAR=RVAR/SVLVOT
Pitfalls of Continuity Method Learning curve of the operator Incorrect placement of sample volume Incorrect annulus measurement Requires 4 separate measurements Introduces 4 possible errors Diameters are squared in the equation so any small error will be magnified and spoil the result Invalid with multivalvular regurgitation or intracardiac shunts