Download

1 / 85
1.13k likes | 2.72k Views
Aortic Regurgitation. Ali Mahajerin Echo Conference September 17, 2008. Introduction. Aortic regurgitation (AR) is characterized by diastolic reflux of blood from the aorta to the LV.

E N D
Aortic Regurgitation Ali Mahajerin Echo Conference September 17, 2008
Introduction • Aortic regurgitation (AR) is characterized by diastolic reflux of blood from the aorta to the LV. • AR may be caused by malfunction of the aortic valve leaflets themselves, by dilation of the aortic root and annulus, or a combination of these factors. • Aortic root disease now accounts for >50% of all AVRs • Clinical presentation is highly variable and depends on multiple factors, including acuity of onset, aortic and LV compliance, hemodynamic conditions, and severity of the lesion.
Epidemiology • Incidence of clinically significant AR increases with age • Typical peak in 4th to 6th decade of life • More common in men than women • Overall prevalence of AR was 4.9% in Framingham Heart Study and 10% in Strong Heart Study • Prevalence of moderate or greater severity was 0.5% and 2.7%, respectively • Most common cause of AR in developing countries is RHD • In developed countries the leading cause of AR is either congenital (particularly due to bicuspid leaflets) or degenerative disease (including annuloaortic ectasia).
Valve-Related Causes of AR • Rheumatic disease • Cusps become fibrotic and retract (usually also stenotic); MV involved as well • Atherosclerotic degeneration • Infective endocarditis • Leaflet perforation • Vegetation interferes with coaptation • Trauma (chest wall or deceleration injury) • Bicuspid aortic valve (can be associated with aortic root dilation as well)
Other Valve-Related Causes of AR • Myxomatous degeneration • Structural deterioration of bioprosthesis • Other less common causes: • Ankylosing spondylitis (can cause disease of both the leaflets and the aortic root) • SLE, RA • Takayasu disease • Anorectic drugs • Membranous subaortic stenosis
Aortic Root Disease Dilation here is common; especially in AS; does not lead to AR • Between the annulus and the ascending aorta is a collagenous segment that forms the sinuses of valsalva. As little as 2mm of dilation here can cause AR Dilation here is rare
Aortic Root Disease • Dilation of the aortic ridge eliminates the normal overlap of the valves
Aortic Root-Related Causes of AR • Idiopathic aortic root dilation • Aortoannular ectasia • Marfan syndrome • Ehlers-Danlos syndrome • Osteogenesis imperfecta • Aortic dissection • Syphilitic aortitis • Trauma • Ankylosing spondylitis • Bicuspid aortic valve with dilated aortic root
Acute Aortic Regurgitation • Most commonly caused by bacterial endocarditis, aortic dissection, or blunt chest trauma • Sudden large regurgitant volume is imposed on an LV of normal size that has not had time to accommodate the volume overload. • Abrupt increase in LVEDV leads to rapid and dramatic increase in LVEDP and LA pressures • Inability of ventricle to develop compensatory chamber dilatation acutely results in a decrease in forward stroke volume. • Tachycardia may develop as a compensatory mechanism to maintain cardiac output, but often insufficient.
Acute AR - Pathophysiology • Patients often present with pulmonary edema or cardiogenic shock. • May present with myocardial ischemia: As LVEDP approaches diastolic aortic and coronary pressures, myocardial perfusion pressure in the subendocardium is diminished. • LV dilation and thinning of LV wall result in increased afterload, and combined with tachycardia leads to increased myocardial O2 demand • Ischemia and its consequences, including sudden death, occur commonly in acute AR.
Chronic Aortic Regurgitation • Chronic AR imposes both volume and pressure overload on the LV. • Increased regurgitant volume increased LVEDV and increased wall stress • Increased chamber compliance accommodates increased volume w/o increasing filling pressures • Compensatory eccentric hypertrophy also occurs, helping to maintain normal stroke volume with the chamber enlargement • LVEDV increases but LV wall compliance prevents increase in LVEDP
Early Compensated Enlarged chamber size ↑ afterload hypertrophy of LV which preserves compliance normal filling pressures LVH ↑ LV mass normal LV vol/mass ratio & EF Progressive LV dilation and systolic HTN ↑ wall stress and vol/mass ratio ↑ wall stress eventually leads to overt LV dysfunction. Decompensated LV systolic dysfunction accompanied by decreased LV diastolic compliance due to hypertrophy and fibrosis Leads to high filling pressures and CHF symptoms Exertional dyspnea common; angina can occur due to reduced coronary flow reserve with predominantly systolic coronary flow Chronic AR - Pathophysiology
Different Stages of AR Bekerdjian R, et al. Circulation 2005; 112: 125-134.
Physical Exam - Auscultation • A2 often soft/absent, P2 normal • S3 if LV function severely depressed • High frequency decrescendo diastolic murmur over the 3rd or 4th intercostal space at left sternal border • Best heard sitting up, leaning forward at end expiration • Austin Flint murmur: mid-to-late diastolic apical rumble, possibly due to vibration of anterior mitral leaflet as it is struck by a posteriorly directed AR jet.
Physical Exam – Peripheral Findings • Corrigan’s pulse – bounding “waterhammer” carotid pulse • deMusset’s sign – head bob with each heart beat • Mueller’s sign – systolic pulsation of uvula • Traube’s sign – pistol shot pulse over the femoral artery • Duroziez’s sign – systolic and diastolic bruits heard when femoral artery partially compressed • Becker’s sign – visible pulsations of retinal arteries and pupils • Hill’s sign – popliteal cuff systolic pressure exceeding brachial pressure by more than 60 mmHg • Mayne’s sign – more than 15 mmHg decrease in diastolic blood pressure with arm elevation • Rosenbach’s sign – systolic pulsations of the liver • Gerhard’s sign – systolic pulsations of the spleen
Natural History of AR • Depends on AR severity, aortic root pathology, and adaptive response of LV. • Bonow et al: • 104 asymptomatic patients with severe AR and normal LVEF • Death, symptoms, or asymptomatic LV dysfunction was < 5%/year over 11-year follow-up • Rate of sudden death was only 0.4%/year • At 11 years, 58% remained asymptomatic and had normal LV systolic function. • Further strengthened serial changes in LV systolic function and/or LV dilatation as important to clinical outcome in AR and potential reasons for AVR. Bonow RO, et al. Circulation 1991; 84: 1625-1635.
Natural History of AR • Dujardin et al: • 246 patients with moderate-severe AR, mean follow-up 7 years • Not all asymptomatic with normal LV systolic function • Ten-year mortality rate 34% • Independent predictors of survival were age, functional class, comorbidity index, atrial fibrillation, LVESD, and LVEF Dujardin KS, et al. Circulation 1999; 99: 1851-1857.
Asymptomatic patients with normal LV function generally have a favorable prognosis • Decline in LVEF with exercise or serial follow-up identifies patients who will likely require surgical intervention. • Even moderate symptoms or evidence of LV dilatation are at higher risk and should be considered for early intervention. Dujardin KS, et al. Circulation 1999; 99: 1851-1857.
Diagnostic Tools: ECG • LVH with or without strain pattern, LAD, LAE • One study suggests that in asymptomatic or mildly symptomatic patients with pure AR, the absence of ECG changes predicts LV systolic dimension < 55mm, and LVEF >45% and >40% with exercise. • Up to 83% of patients with rest or exercise ST segment abnormalities had an enlarged LV (>55mm) or reduced LVEF < 45%. • Conduction abnormalities rare except in late disease with severe LV dysfunction; sustained SVT or VT unusual in absence of significant LV dysfunction.
Chest X-Ray • Cardiomegaly • Prominent Left Ventricle • Ascending Aortic dilatation • LAE only if severe LV dysfunction
Echocardiography • Most important diagnostic test for evaluation of AR as well as for serial follow-up • Allows for: • Assessment of the anatomy of the aortic leaflets and the aortic root • Detection of the presence and severity of AR • Characterization of LV size and function
M-Mode Echocardiography • The aortic regurgitation jet can cascade across the anterior mitral leaflet • Creates a high-frequency fluttering of the anterior mitral leaflet • Increased duration between E and A peaks • Increased distance between the maximal anterior motion of the mitral valve in early diastole (E point) and the most posterior motion of the interventricular septum (e.g., increased E-point septal separation [EPSS]) • In acute AR, premature closure of the MV can also be seen by M-mode • Due to rapidly increasing LV pressure
AR by 2D Echo • 2D Echo will give you a detailed evaluation of the aortic valve and root • Detailed evaluation of LV size and function • Many important causes of AR easily seen on 2D imaging • Even when AR is severe, sometimes 2D imaging is surprisingly normal • Indirect signs of AR: • Diastolic curving of anterior mitral leaflet with concavity towards ventricular septum due to the direct effect of the regurgitant jet
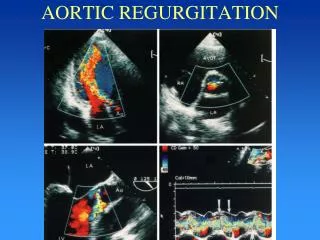
Dilated aortic root due to aortoannular ectasia Large, mobile vegetation Bicuspid aortic valve with characteristic elliptical opening Acute AR due to aortic dissection Bekerdjian R, et al. Circulation 2005; 112: 125-134.
Color Flow Doppler • Color flow jet composed of 3 distinct segments: • Proximal flow convergence zone = area of flow acceleration into the orifice • Vena contracta = narrowest and highest velocity region of the jet at or just downstream from the orifice • The jet itself occurs distal to the orifice in the LV cavity • Measurement of the jet area or penetration into the LV cavity is not accurate in assessing AR severity, though: • If jet width/LVOT width < 25% specific for mild AR • If jet width/LVOT width > 65% specific for severe AR • This works best when regurgitant orifice is relatively round in shape.
Color Flow Doppler • Color flow Doppler is the most common technique to visualize AR • Sensitivity > 95% • False negatives can occur in tachycardia with mild AR • Frame rate allows only a few diastolic frames to be displayed • Can be overcome by using CW -- has a higher sampling rate • Specificity ~100% • Detects even trivial AR • 1% of subjects under age 40 • 10-20% of patients greater than age 60
Eccentric AR jet Width measured at origin of jet adjacent to leaflets Jet width/LVOT width is <25% Case of mild AR Jet width/LVOT width > 65% Case of severe AR Bekerdjian R, et al. Circulation 2005; 112: 125-134.
Vena Contracta • The narrowest diameter of flow stream • Independent of volume flow rate and driving pressure, relatively unaffected by instrument settings • Narrow range of values though, so care needed to obtain optimal images. Ideal sample is: • Perpendicular to jet width • In zoom mode • Narrow sector • Minimum depth • For AR, vena contracta can be measured in parasternal long-axis view preferably in zoom mode.
Vena Contracta • Vena contracta width of ≥ 6 mm correlates well with severe AR (sensitivity 95%, specificity 90%) • Vena contracta width of < 3 mm specific for mild AR. Enriquez-Sarano M, et al. NEJM 2004; 351: 1539-1546.
Proximal Isovelocity Surface Area • Acceleration of flow occurs proximal to the valve plane with a series of isovelocity “surfaces” leading to the high-velocity jet in the regurgitant orifice. • Velocity for a PISA can be determined as the aliasing velocity where a distinct red-blue interface seen (at this interface, velocity is equivalent to Nyquist limit). • Assuming a hemispherical shape, the surface area of the PISA region is 2πr2 • Peak regurgitant flow obtained by multiplying surface area by aliasing velocity, and effective regurgitant orifice area (EROA) is peak regurgitant flow divided by peak velocity obtained by CW Doppler.
PISA - Limitations • Isovelocity contour flattens as it approaches the orifice, underestimating flow • Proximal structures can distort the isovelocity contour • Sensitive to errors in radius measurement • 10% error in radius leads to 21% error in flow
Continuous Wave Doppler • Because AR jet is high velocity, CW Doppler necessary to record envelope of jet. • Several types of info can be derived: • Antegradeflowvelocity • Signal intensity relative to antegrade flow • Time course (shape) of velocity curve • AR results in increased antegrade volume flow rate across AV, which is reflected in an increase in the antegrade velocity across the valve. • The greater the severity of AR, the higher the antegrade velocity across the AV • Must also consider possibility of coexisting AS
Signal intensity is proportional to # RBCs contributing to regurgitant signal. • Can compare intensity of regurgitant signal to antegrade flow as a qualitative estimate of regurgitant severity. • Weak signal reflects mild severity; signal nearly equal to antegrade flow reflects severe regurgitation. AR Antegrade
CW Doppler: Pressure Half-Time • Shape of AR velocity curve depends on time course of diastolic pressure difference across AV • Chronic severe AR results in increased aortic pulse pressure with low aortic EDP. Rapid rate of decline in aortic pressure is reflected in steeper diastolic deceleration slope (even if LVEDP remains low). • Thus, diastolic deceleration slope provides a semiquantitative measure of AR severity. • A flat slope (P1/2 > 500 msec) is consistent with mild AR, and a steep slope (P1/2 < 200 msec) indicates severe AR. • For a given severity of AR, P1/2 will be shortened by elevated LVEDP or vasodilator therapy that reduces AR.
Pressure Half-Time • With acute AR, LV compliance has not yet adapted leading to significant increase in LVEDP. In extreme cases, aortic and LV EDP may equalize at end-distole, resulting in a triangular-shaped CW-Doppler with linear deceleration slope from maximum velocity to baseline. • Limitations of pressure half-time assessment: • Pressure half-time sensitive to chronicity of AR • Acute AR leads to much shorter values than chronic AR when LV is dilated with increased compliance • Pressure half-time varies with SVR • Vasodilators may shorten the pressure half-time even as the aortic regurgitant fraction improves.
Regurgitant Volume or Fraction • Can compare flow through AV versus MV or PV • Stroke volume at any valve annulus is derived as the product of CSA and VTI of flow at the annulus • In the absence of regurgitation, SV determinations at different sites (LVOT, mitral annulus, pulmonic annulus) should be equal • In the presence of regurgitation of one valve, without any intracardiac shunt the flow through the affected valve is larger than the other valves • RV is the difference between the two flows • RF is the RV divided by forward stroke volume through the regurgitant valve.