Download
1 / 1

E N D
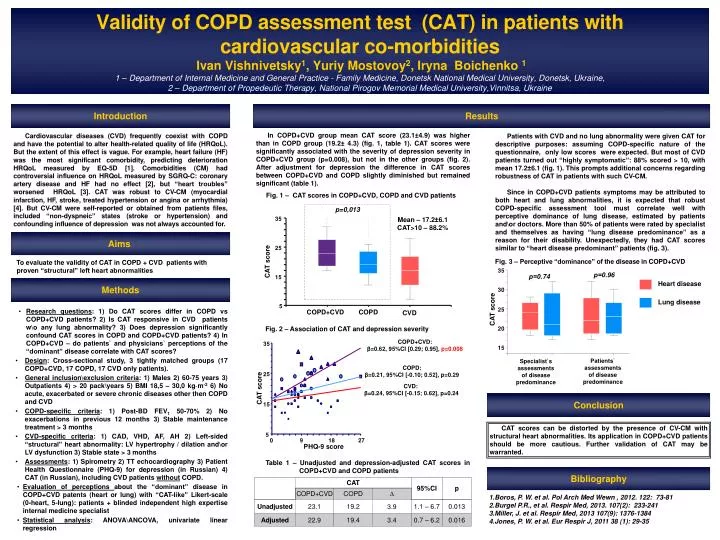
Validity of COPD assessment test (CAT) in patients with cardiovascular co-morbiditiesIvan Vishnivetsky1, Yuriy Mostovoy2, Iryna Boichenko 11 – Department of Internal Medicine and General Practice - Family Medicine, Donetsk National Medical University, Donetsk, Ukraine,2 – Department of Propedeutic Therapy, National Pirogov Memorial Medical University,Vinnitsa, Ukraine 35 25 15 5 0 9 18 27 Introduction Results In COPD+CVD group mean CAT score (23.1±4.9) was higher than in COPD group (19.2± 4.3) (fig. 1, table 1). CAT scores were significantly associated with the severity of depression severity in COPD+CVD group (p=0.008), but not in the other groups (fig. 2). After adjustment for depression the difference in CAT scores between COPD+CVD and COPD slightly diminished but remained significant (table 1). • Cardiovascular diseases (CVD) frequently coexist with COPD and have the potential to alter health-related quality of life (HRQoL). But the extent of this effect is vague. For example, heart failure (HF) was the most significant comorbidity, predicting deterioration HRQoL measured by EQ-5D[1]. Comorbidities (CM) had controversial influence on HRQoLmeasured by SGRQ-C: coronary artery disease and HF had no effect [2], but “heart troubles” worsened HRQoL[3]. CAT was robust to CV-CM (myocardial infarction, HF, stroke, treated hypertension or angina or arrhythmia) [4]. But CV-CM were self-reported or obtained from patients files, included “non-dyspneic” states (stroke or hypertension) and confounding influence of depression was not always accounted for. Patients with CVD and no lung abnormality were given CAT for descriptive purposes: assuming COPD-specific nature of the questionnaire, only low scores were expected. But most of CVD patients turned out “highly symptomatic”: 88% scored > 10, with mean 17.2±6.1 (fig. 1). This prompts additional concerns regarding robustness of CAT in patients with such CV-CM. Since in COPD+CVDpatients symptoms may be attributed to both heart and lung abnormalities, it is expected that robust COPD-specific assessment tool must correlate well with perceptive dominance of lung disease, estimated by patients and\or doctors. More than 50% of patients were rated by specialist and themselves as having “lung disease predominance” as a reason for their disability. Unexpectedly, they had CAT scores similar to “heart disease predominant” patients (fig. 3). Fig. 1 – CAT scores in COPD+CVD, COPD and CVD patients p=0,013 Mean – 17.2±6.1 CAT>10 – 88.2% 35 Aims 35 р=0.96 р=0.74 25 • Heart disease 30 • CAT score Fig. 3 – Perceptive “dominance” of the disease in COPD+CVD • To evaluate the validity of CAT in COPD + CVD patients with proven “structural” left heart abnormalities • Lung disease • CAT score 15 25 Methods 20 5 • Research questions: 1) Do CAT scores differ in COPD vs COPD+CVD patients? 2) Is CAT responsive in CVD patients w\o any lung abnormality? 3) Does depression significantly confound CAT scores in COPD and COPD+CVD patients? 4) In COPD+CVD – do patients` and physicians` perceptions of the “dominant” disease correlate with CAT scores? • Design: Cross-sectional study, 3 tightly matched groups (17 COPD+CVD, 17 COPD, 17 CVD only patients). • General inclusion\exclusion criteria: 1) Males 2) 60-75 years 3) Outpatients 4) > 20 pack\years 5) BMI 18,5 – 30,0 kg·m-2 6) No acute, exacerbated or severe chronic diseases other then COPD and CVD • COPD-specific criteria: 1) Post-BD FEV1 50-70% 2) No exacerbations in previous 12 months 3) Stable maintenance treatment > 3 months • CVD-specific criteria: 1) CAD, VHD, AF, AH 2) Left-sided “structural” heart abnormality: LV hypertrophy / dilation and\or LV dysfunction 3) Stable state > 3 months • Assessments: 1) Spirometry 2) TT echocardiography 3) Patient Health Questionnaire (PHQ-9) for depression (in Russian) 4) CAT (in Russian), including CVD patients withoutCOPD. • Evaluation of perceptions about the “dominant” disease in COPD+CVD patents (heart or lung) with “CAT-like” Likert-scale (0-heart, 5-lung): patients + blinded independent high expertise internal medicine specialist • Statistical analysis: ANOVA\ANCOVA, univariate linear regression COPD+CVD COPD CVD 15 Fig. 2 – Association of CAT and depression severity • Patients` assessments • of disease predominance • Specialist`s assessments • of disease predominance • COPD+CVD: • β=0.62, 95%CI [0.29; 0.95], p=0.008 Conclusion COPD: β=0.21, 95%CI [-0.10; 0.52],p=0.29 CAT scores can be distorted by the presence of CV-CM with structural heart abnormalities. Its application in COPD+CVD patientsshould be more cautious. Further validation of CAT may be warranted. CVD: β=0.24, 95%CI [-0.15; 0.62],p=0.24 • CAT score Table 1 – Unadjusted and depression-adjusted CAT scores in COPD+CVD and COPD patients Bibliography Boros, P. W. et al. Pol Arch Med Wewn, 2012. 122: 73-81 Burgel P.R., et al. Respir Med, 2013. 107(2): 233-241 Miller, J. et al. Respir Med, 2013 107(9): 1376-1384 Jones, P. W. et al. Eur Respir J, 2011 38 (1): 29-35 PHQ-9 score






















