Download
1 / 1
10 likes | 142 Views
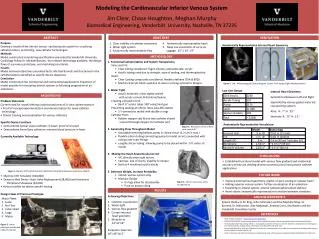
Figure 3. Bifurcation of the inferior vena cava at 60 °. Modeling the Cardiovascular Inferior Venous System Jim Clear, Chase Houghton, Meghan Murphy Biomedical Engineering, Vanderbilt University, Nashville, TN 37235. ABSTRACT. OBJECTIVES. VERIFICATION. Purpose

E N D
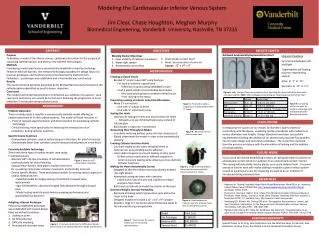
Figure 3. Bifurcation of the inferior vena cava at 60° Modeling the Cardiovascular Inferior Venous System Jim Clear, Chase Houghton, Meghan Murphy Biomedical Engineering, Vanderbilt University, Nashville, TN 37235 ABSTRACT OBJECTIVES VERIFICATION Purpose Develop a model of the inferior venous cardiovascular system for visualizing catheterizations and testing new catheter technologies Methods Model constructed considering specifications presented by Vanderbilt University Cardiology Fellow Dr. Michael Barnett, the relevant technology available, the design flaws of a previous prototype, and machining constraints Results Model achieved objectives presented by Dr. Michael Barnett and functioned in the catheterizations identified as specific device objectives Conclusion Model constructed has commercial and instructional applications. Expansion of model possible for simulating arterial systems or following progression of air embolisms • Clear visibility of catheter movement • Water tight system • Anatomically representative flow • 4. Anatomically representative heart • 5. Meet size constraints of carry-on luggage: 22” x 14” x 9” Anatomically Representative Internal Heart Geometry METHODOLOGY • 1. Functional Catheterization and System Transparency • Veins and IVC: • Clear tubing considered: Tygon silicone, polycarbonate, acrylic • Acrylic tubing used due to strength, ease of sealing, and thermoplasticity • Heart: • Clear Casting compounds considered: flexible urethane (70A & 80D) • Machined acrylic block used due to ease in carving symmetric designs • 2. Water Tight • Acrylic materials: Joints tightly sealed • with acrylic cement & dichloroethylene • Creating a Closed Circuit • Bent ½” acrylic tubes 180° using heat gun • Preventing Leaking at Inferior Vena Cava Bifurcation • 2 Y-connectors sealed with double o-rings • Catheter Ports • Rubber stopper seal & one way catheter sheath • inserted through stopper for catheter port • 3. Generating Flow Throughout Model • Adjustable metering bellows pump in closed circuit (1.2 L/min max ) • Flexible silicon tubing connecting pump to model circuit; connected with clamps over tube fittings • Lengthy silicon tubing allowing pump to be placed within ~5 ft radius of model • 4. Making the Heart Anatomically Correct • IVC directly enter right atrium • Castings- lack of clarity, inability to release • Built as 4 machined acrylic blocks • 5. Decrease Weight, Increase Portability • Inferior venous system only • Modular Design • O-rings allow for disassembly • Push on pump tubing Figure 5. Left:Mid esophageal Echocardiogram Center: ProE design Right: Machined Heart Low Cost Design Internal Heart Geometry Symmetrical between Left and Right Separated by various gasket materials representing septum Atria: R: .7” H: .75” Ventricle: R: .75” H: 1.2” BACKGROUND • Problem Statement • Current need for model offering unobstructed view of in vitro catheterizations • Proof of concept experimentation and demonstration for novel catheter technology • Clinical training and visualization for various catheters • Specific Device Functions • Demonstrate optical scope catheters in heart: proof of concept • Demonstrate Swan-Ganz catheters: measure blood pressure in heart • Currently Available Technology < ≈60° Anatomically Representative Vasculature CONCLUSIONS • Established functional model with venous flow gradient and anatomical accuracy at low cost yielding diverse commercial and instructional catheter applications Figure 1. Mentice VIST (left) & Dynamic Med Demo Peripheral Showcase Interactive (Right) FUTURE WORK • Mentice VIST Simulator ($40,000) • Dynamic Med Demo- Heart Valve Replacement ($8,000) and Interactive Peripheral Showcase ($4,000) • Various models for device specific testing • Improve external heart geometry: plaster of pariscasting of cadaver heart • Adding superior venous system: further visualization of air embolism • Expanding to arterial system: arterial catheterizations/stent delivery • Heart valves: anatomically representative transition between chambers Figure 4.Inferior vena cava entry to right atrium RESULTS Design Flaws of Previous Prototype Achieving Objectives: Catheter visualization Water tight Venous flow gradient Correct internal heart geometry Modular to 13’’x6’’x6’’ Exception: base size 28’’x16’’x6.5’’ ACKNOWLEDGEMENTS Major Flaws: 1. Leaks 2. No Flow 3. Cubic Heart 4. Large 5. Messy Special thanks to Dr. King, John Fellenstein and the Machine Shop, Dr. Barnett, Dr. Merryman, Alex Makowski, Andrew Cross, Ray Booker and the Vanderbilt Simulation Center 2. REFERENCES 4. 1. • CESEI. Patient Simulators. <www.cesei.org/simulators.php> • DYNAMIC MED DEMO. Demonstration Devices for the Medical Industry. <http://www.dynamicdemo.net/anatomical.html> • Hertzberg BS, Kliewer Ma, Delong DM et al. Sonographic Assessment of Lower Limb Vein Diameters: Implications for the Diagnosis and Characterization of Deep Venous Thrombosis. AJR. May 1997; 168:1253-1257. • Pantalos GM, Koenig SC, Gillar KJ, Giridharan GA, Ewert DL. Characterization of an adult mock circulation for testing cardiac support devices. ASAIO. Feb 2004; 50(1):37-46. • Short N. Technical and Historical Perspectives of Remote Sensing. <http://www.fas.org/irp/imint/docs/rst/Intro/Part2_26d.html> 3. Figure 2. Initial prototype established under Dr. Barnett