Download
1 / 44
440 likes | 601 Views
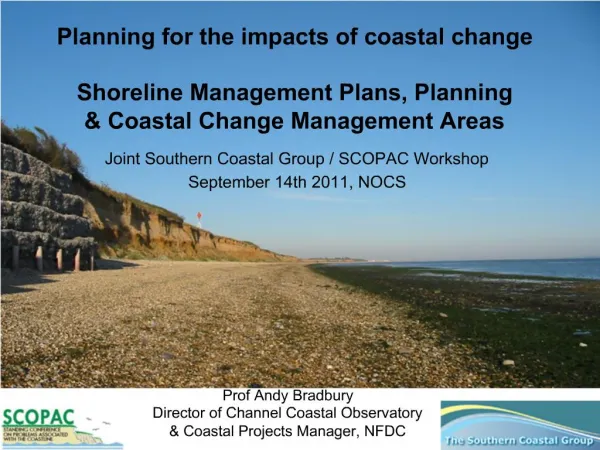
Planning an effective Change Management Programme appropriate to the NHS. Yi Mien Koh Chief Executive Thursday 2 April 2009. Agenda. Background Hillingdon’s story Strategic objectives Key developments Gaps and challenges Risks The future vision. Background.

E N D
Planning an effective Change Management Programme appropriate to the NHS Yi Mien Koh Chief Executive Thursday 2 April 2009
Agenda • Background • Hillingdon’s story • Strategic objectives • Key developments • Gaps and challenges • Risks • The future vision
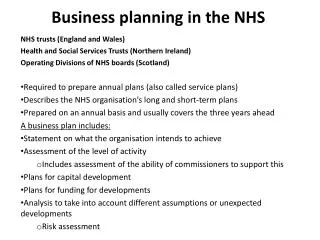
Hillingdon health system key facts PCT 2008/9 budget £330m (before deficit repayment) Resident population 250,000. Registered population 265,000 49 GP practices with 200 GPs 62 pharmacies 42 dental practices with 150 GDPs 47 Optometric practices The Hillingdon Hospital NHS Trust (and Mount Vernon Treatment Centre) Harefield Hospital (Royal Brompton & Harefield NHS Trust) Mount Vernon Cancer Centre (East & North Herts NHS Trust) Hayes Cottage Hospital Renal Unit (Imperial Healthcare NHS Trust) Central & North West London Mental Health FT BMI Healthcare at Mt Vernon PCT Provider Services 352 (CATS provider) ISTC (InHealth and Clinicentre) The Practice plc (CATS) Hillingdon Health Limited (PBC/Harmoni Joint Venture) Voluntary sector Health and Social Care
History • First wave PCT in country, established Feb 2000 • Poor commissioning in a monopolistic provider driven system • Never in balance, largest deficit in NHS history, Public Interest Report • 6 CEs, 3 Chairs, 4 FDs in two years (2005/7) • No recognition of health inequalities and investment driven by the articulate • Failed Fitness for Purpose and KPIs in 2006/7 • New CE, new chair, new board - 2007
The story ........ is how we systematically turned around the PCT in a journey of improvement over three years to reach level 2 on WCC competencies Headline successes: • Breakeven (first time in 7 years) • Performance on national KPIs - top quartile of PCTs in London • Paid off £18m of legacy debt (annual repayment £8m plus £1m interest) • On target to clear deficit by 2011 • FESC procurement • Clear strategy
North West London Primary Care Trusts Spend by PCT 2006/07 (£m) Sector average 43% Hillingdon 54%
NHSL 2007/8 Outturn Performance on 18 weeks, A&E, MRSA & Finance 19 PCTs achieved 18 weeks admitted; 25 PCTs achieved 18 weeks non-admitted; 15 PCTs achieved A&E (source: weekly sitreps); 9 PCTs (of 27) achieved MRSA trajectories; 21 PCTs achieving finance control total 4 PCTs ‘green’ on all 18 weeks subject to meeting DH data completeness check
Journey to Becoming World Class 2011/12 World Class (self care/ prevention) Debt free Strategy implemented Improvement in health and health outcomes Focus: continuous quality improvement and innovation Goal: strong, vibrant local health economy providing high quality care 2009/10 Consolidation (outpatients) Embedding existing achievements Maintaining breakeven Focus: strategy (implementation), contracts (out of hospital), PBC, OD (succession planning), joint working with La and other PCTs Goal: sustainability 2008/9 Recovery ( high dependency to wards) Maintaining 07/08 achievements FOT breakeven Provider development - FT, APO Performance (AHC)- top quartile (Q2, NHSL) Focus: finance, strategy (development), contracts (acute), PBC, market stimulation, PPE Goal: embeddedness 2007/8 Turnaround (critical care) Achieved breakeven Evidence based decisions culture Substantive chair, CE, FD, new board ALE score = 2 Performance - top 7 PCTs in London Focus: finance, controls, relationships, commissioning, performance Goal: meeting statutory duty 2006/7 Annus horribilis(Crash) £53m deficit Organization failure public interest report Interim chair, CE, FD Incomplete FFP Poor relationship with stakeholders Nil credibility Information free zone Financial Performance (£) WCC Competency levels 2002 first reported deficit Baseline Budget -£53M -£43M -£19M -£153k -£35M -£27M £0M 2009/10 2010/11 2011/12 2002 2006/7 2007/8 2008/9
Fundamental strategy Identifying and tackling underlying reasons for poor performance and building from clinically-led evidence base Enablers Clear strategy Proactive relationship with opinion formers New values Embracing and managing GPs and clinicians Performance management Knowledge based decision making Systematise processes Strengthening commissioning Strategic partnership with LA Improvement and innovation Sustainability
PCT strategy Shifting the system towards self care and prevention Hospital services Health & Wellbeing Primary & Community care Self care direction of travel for service & resource shifts over next five years
Strategic objectives • Sustaining financial balance • National priorities and healthcare standards • PCT (vital signs) and LSP priorities • Pegging hospital activities and investing in out of hospital services • Tackling inequalities by investing in south
CSP priorities (based on JSNA) • Investments to target families in south of the borough. Progress to be monitored by life expectancy and all age all cause mortality • Improve maternity care to improve outcomes for mothers and their babies as measured by birth weight and breast feeding rates • Improve health and wellbeing of children, in particular children in need, to reduce teenage pregnancies and to improve educational attainment • Obesity care pathways for children and adults • CHD prevention, including diabetes, in targeted populations by commissioning preventive services such as smoking cessation and exercise • Improve employment opportunities and general healthcare for people with mental ill health
Journey to World Class Commissioning 1. Leadership Problem – nil credibility Progress - proactive programme of engagement with MPs and LA – honest listening and strategic; involving them along the journey of improvement 2. Partnership Problem – health not on agenda, little influence on LSP and frozen out of developments in borough Progress – health number one priority of LSP, excellent joint working, co-location at Civic and joint DPH. Children’s Centres, Building Schools for the Future and integration of services in polyclinics
World Class Commissioning competencies (cont) 3. Patient and public engagement Problem – little engagement except from the articulate. No strategy and resources Progress – PPE strategy 4. Clinical engagement Problem – little clinical engagement, poor relationship with GPs, consultants and predominantly administrative approach Progress – PEC re-established. PBC initiatives: Urgent Care Centre, Referral Management Centre, PBC Director. Hillingdon Health Ltd. 5a. Needs assessment Problem – public health not integrated into PCT or LSP Progress – Joint Strategic Needs Assessment driving LSP and PCT priorities
Figure12 : Index of Multiple Deprivation (2007) by all, children and older people in Hillingdon (Super output area relative to England)
Hillingdon Borough geo-coded crimes between 19/11/2007 and 18/11/2008 (Domestic Violence) I 50 F 38 F 35
Example of needs assessment and knowledge managementCoronary Heart Disease
World Class Commissioning competencies (cont) 5b. Knowledge management Problem – information and knowledge free zone Progress – tripled size of analytical team. Care and resource utilisation review ( Department of Health CRU model) including benchmarking. Internalised BUPA’s clinical insights informing claims management and care pathways. Polyclinic modelling. Modelling impact of tariff reforms. Key achievements - Demand management initiatives: Rapid Response, Case Management, UCC, RMC, CATS. Performance management and validation routines (13) adopted by all NWL PCTs. Trainers for Healthcare for London polyclinic modelling – training other PCTs. Insights of FESC procurement shared with PCTs around the country
Predictive modelling of CHD prevalence in Hillingdon 2005-2020
BUPA Clinical Appropriateness Rules Engine Admission for non-clinical reasons Incorrect dominant procedure Invalid dominant diagnosis Admission of patients who could have been treated without the need for admission to hospital, or within a 4 hour period. The coding of the incorrect primary procedure based on the care the patient received, causing the wrong HRG to be applied. The coding of a secondary/ comorbid diagnosis in the primary diagnosis field, causing the wrong HRG to be applied. Complication of procedures Inappropriate coding of an admission to hospital, the Primary diagnosis should have been a complication of procedure. Irrelevant Co-morbidity Coding Low Priority Procedures Underlying diagnosis dominant Coding of co-morbidities that do not impact the clinical management or resource use, artificially inflate the HRG to a more complex level. The coding of a patients diagnosis leading to admission in a field other than the primary diagnosis, causing the wrong HRG to be applied. Patients given a treatment contractually identified as Low Priority, without the required pre-approval from the PCT.
World Class Commissioning competencies (cont) 6. Prioritise investment Problem – spends not aligned to needs due to lack of strategy Progress – Commissioning Strategy Plan priorities identified by JSNA and predictive modelling supported by Medium Term Financial Plan 7. Market stimulation Problem – monopolistic provider Progress – Provider map. Procurement: FESC, CATS, UCC, RMC, EPIOCS (wheelchairs), diabetic screening, GP-led Health Centre
World Class Commissioning competencies (cont) 8. Improvement and Innovation Problem – information and knowledge free zone Progress – Use of information to inform strategic decision making. Pilot for NHS Institute tool for improvement opportunities, RMC, clinical assessment panel and extended clinical assessment clinics. BUPA care pathway redesign. Benchmarking of programme budgets and outcomes. Advanced data validation of claims management. Key developments – Contracting with ICHT for packages of care for chronic kidney disease. JV with London Deanery to run masterclasses for GPs on RMC hot topics and developing community specialist workforce. Feedback to GPs from consultant panel on referral quality to support development and improvement, GP balance scorecard includes benchmarking gatekeeper role. Testing of new pathways in community assessment clinics to refine specifications for procurement.
AS SHOULD BE AS IS IN IN HILLINGDON HILLINGDON 1150 patients a year turn up at GP Surgeries 6 months wait 1150 patients a year turn up at GP Surgeries 73 being referred for Outpatient Care (+ possible 736 ( 64 %) should require 18 weeks ( max ) Nerve Conduction Testing ) 18 weeks ( max ) Nerve Conduction Testing 90 + 44 receiving Physio 205 Surgery ( 18 %) 736 Surgery ( 12 %) ? 736 Physio Rehab 205 Physio Rehab Carpal Tunnel: how patients funnel down from GPs to Outpatients and then to Inpatients/Surgery The following diagram contrast a years worth of activity and cost associated with ‘as is’ Hillingdon activity (on the left) to ‘ideal – best in class’ activity and costs (on the right)
Analysis of GP referrals April- Oct 2008(Hillingdon PCT Referral Management Centre)
Referral Management Centre ( RMC) • Established Jan 2008 – a PBC initiative • Processes 50,000 referrals a year – GP (75%) and non urgent intra-hospital (25%) or C2C referrals • Web-based referral tracking system (Amazon style) – paperless via Choose and Book • Most referrals triaged by consultants covering 8 highest volume specialities • Turnaround max 48 hours • Near real time monitoring of referral activity • Clinical insights into volume and quality of GP referrals • Annual (body shop) running cost: £650,000
Clinical Assessment Panel • PCT employs a panel of NHS consultants (and GPSIs) in twilight years of career covering 8 high volumes specialties • Remote working, guaranteed max 48 hours triage. Must agree to be contactable by GPs in office hours. Pay £100/hr • Triage options: advice back to GP (5%), referral to consultant community assessment clinics (20%), referral to allied health professionals (5-15%), referral to diagnostics (20%), approval for onward referral to hospital (50%) • Community Assessment Clinics in six specialties: musculoskeletal (MSK), dermatology, gynaecology, ophthalmology, cardiology, ENT • Example: MSK: Patient satisfaction survey – 100%. Service quadrupled in 4 months due to patient demand. Savings: 250k since July 2008.
World Class Commissioning competencies (cont) 9. Procurement skills Problem – poor procurement history due to lack of expertise Progress – Procurement Strategy. Commercial Director appointed. NHS London commercial strategy. London clinical and business support Agency (Hub) 10. Health system management Problem – ineffectual commissioner in monopolistic provider driven system Progress – contract management of all types of providers in a well performing health economy 11. Investment strategy Problem – short term focus and no financial strategy Progress – medium term financial plan
Gaps and challenges • Legacy debt • Organizational capacity and capabilities • Clinical engagement • Poor primary care infrastructure • Competing (top down) priorities • Provider resistance • Regulation • Flat health budget from 2011 • Pace of change and execution
Risks • Not breaking even • Demand management • Clinical engagement • Not achieving efficiency targets • Relationship with providers • Tariff reforms (MFF, HRG4) • Succession planning • PCT mergers or reconfigurations • Strategy execution
Risk mitigations • Medium term financial plan • Robust demand and activity planning including modelling impact of new tariffs and alignment between finance and activity plans • Demand management strategies • Refreshed PEC and PBC • Outer NWL acute commissioning alliance • London clinical and business support agency • Alignment with WCC principles
What would success look like in 5 years ? • Investment returns show VFM and improved health outcomes • Strong vibrant health economy • Reducing health inequalities • Plurality of providers and patient choice • PCT as health system manager and driver of improvement and innovation • Recognized by partners and population as local leader of the NHS • Summary of journey of improvement (next page)