Download
1 / 26
510 likes | 3.84k Views
Pathophysiology of Hypertension. Tatár M. Dept. of Pathophysiology Jessenius Med. School. - venous return - extracellular fluid volume - myocardial contractility. - vasoactive substances thickening of arteriolar wall. Essential Hypertension.

E N D
Pathophysiologyof Hypertension Tatár M. Dept. of Pathophysiology Jessenius Med. School
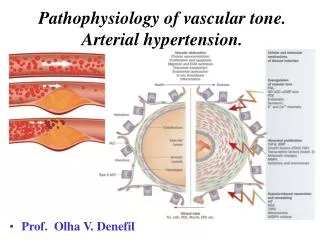
- venous return - extracellular fluid volume - myocardial contractility • - vasoactive substances • thickening of arteriolar • wall
Essential Hypertension • Hemodynamic effect of hormonal, neural and renal dysregulation of blood pressure • Pathogenesis is probably a slow and gradual process • No single or specific cause • Initiating factors may no longer be apparent when hypertension is developed, since they have been „normalised“ by the compensatory interactions • Initial phase: cardiac output • Late phase: peripheral arteriolar resistance, cardiac output is normalised
INCREASED EXTRACELLULAR FLUID VOLUME INCREASED BLOOD VOLUME INCREASED VENOUS RETURN INCREASED CARDIAC OUTPUT AUTOREGULATION INCREASED TOTAL PERIPHERAL RESISTANCE INCREASED BLOOD PRESSURE
Mechanisms of EH • activity of renin-angiotensin-aldosteron • Hyperfunction of sympathetic system • Vasoactive substances - endothelial dysfunction • Insulin resistance obesity • Arteriolar hypertrophy • Renal defect to excrete sodium
Increased R-A-A activity ANGIOTENSINOGENE RENIN J-G ACE ANGIOTENSINII ANGIOTENSINI ALDOSTERON VASOCONSTRICTION Na+ RETENTION negativefeed back BLOOD PRESSURE
Tissue R-A system (Beevers et al., 2001) • - catecholamine and endothelin release • induction of hypertrophy of smooth muscle cells, • cardiomyocytes
Hyperfunction of sympathetic system • Primary activity of vasomotor neurons • Angiotensin II and endothelin increases activity of vasomotor neurons • Norepinephrine potentiates renin releasing
Vacoactive substances Influence on vascular tone and sodium transport Endothelin Digitalis (ouabain) – like substance Natriuretic peptides
Sodium transport across vascular smooth muscle cell membrane • Sodium retention activation of natriuretic mechanisms • Digitalis - like inhibitor of Na+,K+,ATP-ase
INSULIN RESISTANCE HYPERINSULINEMIA HDL SYNDROME X OBESITY HYPERTENSION VLDL GLUCOSE INTOLERANCE
INSULIN RESISTANCE HYPERINSULINEMIA • SYMPATHETIC ACTIVITY SODIUM RETENTION ARTERIOLAR HYPERTROPHY HYPERTENSION
(tonic activity) Regulatory cells (Reaven et al., 1996)
Hypertrophyof Arteriolar Wall RENAL HYPOPERFUSION STRESS OBESITY Na+ RETENTION NATRIURETIC HORMON INSULIN CATECHOLAMINES ANGIOTENSIN PRESSURE-GROWTH EFFECTS INTRACELLULAR Ca2+ Na+/H+ EXCHANGE SMOOTH MUSCLE CONTRACTION VASCULAR WALL HYPERTROPHY • PERIPHERAL VASCULAR RESISTANCE
Role of Kidneys (Johnson et al., 2002)
Renal Lesions 1st phase- normal kydneys and sodium excretion - sympathetic hyperactivity, R-A stimulation renal vasoconstriction 2nd phase- tubular ischemia - interstitial inflammation - ultrafiltration and Na+ reabsorbtion increased blood pressure 3rd phase- elimination of tubular ischemia; sodium excretion is normal BP is more increased after enhanced salt intake
Right shift of „pressure-natriuretic“ line (Cowley and Roman, 1996)
Conclusions • Interaction between increased activity of sympatihetic and R-A systems and dysregulation of sodium balance and intravascular volume • Endothelial dysfunction – dysbalance between vasoconstrictor and vasodilator agents • Hyperinsulinemia – a) direct effect on sodium retention, b) sympathetic activation through the suppression of regulatory neurons in hypothalamus • Hypertrophy of arteriolar wall – increased vasoconstrictor reactivity • Genetic factors: dysfunction of membrane mechanisms of vascular smooth muscle cells; disorder of sodium exchange in nephron epithelial cells • Acquired renal injury: sodium intake is excreted only with increased blood pressure