Download
1 / 35
350 likes | 400 Views
Explore the significance of airway structural changes in asthma and bronchiectasis, prevalence of comorbidities, diagnostic criteria, and treatment options for intractable asthma.

E N D
Asthma and Bronchiectasis Branislava Milenkovic Professor of Internal/Respiratory Medicine, University of Belgrade Deputy Director of Clinic for Pulmonary Diseases, Clinical Center of Serbia, Belgrade, Serbia
Disclosures 2010 - 2017 Branislava Milenkovic Lectures: AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Novartis, Takeda, TEVA Consultancy or national/regional Advisory Boards: AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis Educational programmes: no Industry-sponsored grants (Institution): no
Airway Structural Changes In Airway Diseases * overall estimate of the significance of these changes in the conditions mentioned Scores: + = mild ++ = moderate +++ = significant ++++ = marked ? = uncertain Bergeron & Boulet CHEST 2006
Bronchiectasis (and asthma) • Asthma (and bronchiectasis) Asthma Bronchiectasis
Bronchiectasis - Comorbidities • Common among bronchiectasis patients at any stage of the disease • Limited data regarding prevalence and impact on disease outcomes • Single disease approach ineffective • Given ageing population, number of comorbidities likely to increase • Associated increase in healthcare costs Adapted from DoH document: A framework of principles for system wide action on comorbidity
Bronchiectasis - Derivation cohort - • 4 European Centres • Galway (Ireland), n=280 • Dundee (Scotland), n=286 • Leuven (Belgium), n= 190 • Monza (Italy), n=230 • Total study population (n=986)
Bronchiectasis (and asthma) A woman with intractable asthma E-mail:branislava.milenkovic@kcs.ac.rs
A woman with intractable asthma - History • 55-years-old lady, house-keeper, non-smoker • Referred for « uncontrolled asthma » • Salmeterol/fluticasone 50/250 mcg bd • Theophylline tbl a 250 mg bd • Salbutamol MDI prn • Asthma – 14 years, 3-4 oral CS courses per year • Diabetes - 20 years, type I • Retinopathia diabetica • Bronchiectasis - 4 years • 2years history of asthma persistent symptoms: • Dry cough • Wheezing episodes • Exertional dyspnea • Night’s wakening • Worsening over the last two months, 3 AB courses (ciprofloxacine, roksitromicin, azithromycine), methzlprednisolone ) with slightly reduced symptoms.
A woman with intractable asthma - 2011. • Examination: • Rr=16/min, Fc=104/min, TA=120/75 mmHg, SAT=94% • Insp& expwheezing. • Sputum: • Pseudomonas, Klebsiella • sensitive:ceftazidime, tazobactam, amikacin,imipenem, meropenem. • Spirometry (post-SeretideR): • FVC=108%, • FEV1=84%, FEV1/FVC=66%. • Body pletismography: • TLC=108%, RV=112%, RV/TLC=37.9%, ITGV=126%, Raw=0,37. • Lab results: • SE=18, • WBC=8,53 (76,8% neutrophils), CRP=5,4, • glucose=16,3 mmol/l, • urine++;ketone negative, • Total IgE=89,6 UI/l.
CT – 2011. CT – 2010.
A woman with intractable asthma - Tx • Ceftazidime2 g t.i.d • N-acetylcysteine • Chest physiotherapy • Fluticasone/Salmeterol500/50 b.d. • Theophyllinetbl a 250 mg bd • Salbutamol MDI100 mcg prn • Sputum: negative • Spirometry (post-SeretideR): • FVC=109%, • FEV1=88%, FEV1/FVC=71%
Severe Asthma Phenotype? Difficult to Treat Asthma? ERS/ATS Task Force ERJ 2013.
A woman with intractable asthma - 2014. Yellow Nail Syndrome
A woman with intractable asthma – 2014/2017 2014. July 2017.
Asthma (and bronchiectasis) • Bronchiectasis (and asthma) Asthma Bronchiectasis
Asthma phenotypes • Allergic / Non-allergic (intrinsic) • Inflammatory phenotypes: eosinophilic, neutrophilic, paucigranulocytic • Asthma in obese adults • Severe asthma • Adult onset asthma • Adult-onset obese female preponderant asthma • Adult-onset non-atopic, inflammation-predominant phenotype with fixed airflow limitation • Adult-onset mild asthma • Smoking-related asthma Laforest L, et al. EurRespir J 2006;27:42-50. de Nijs S, Venekamp LN, Bel EH. EurRespir Rev 2013;22:44-52.
Why is it important to differentiate between asthma phenotypes? • Treatment • Corticosteroids • Disease progress • Fixed airflow obstruction • Genetics of asthma • More accurate disease classification • Aetiology • Causal exposures
Asthma (and Bronchiectasis) A woman with intractable asthma E-mail:branislava.milenkovic@kcs.ac.rs
A woman with intractable asthma • 53-year old nurse • Asthma for 11 years • Ex-smoker • Atopy • Comorbidities: • diabetes mell. • depression • Treatment: • LABA/ICS bid • Berodual MDI prn. • At presentation: • Fr=16/min, Fc=100/min, TA=125/80mmHg, SAT=94%, • prolonged expiration • IgE= 512 kU/L • WBC=9.8 (1% eosionophils) • Spirometry (basal): • FVC=82%, • FEV1=59%, • FEV1/FVC=61% • ACT score = 13; NO= 17 ppm • 4 MDIs (Ventolin) for one year • 1 exacerbation for one year
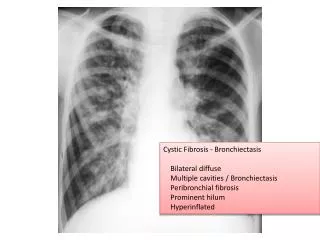
53-year old nurse - At admission Courtesy by Prof. Ruza Stevic
Minimal Diagnostic Criteria for ABPA-Central Bronchiectasis • Asthma • Central bronchiectasis • Immediate cutaneous reactivity to Aspergillus species or A. fumigatus • Elevated total serum IgE (>417 kU/L) - 512 kU/L • Elevated serum IgE-A.fumigatus and or IgG-A.fumigatus compared to sera from prick positive patients with asthma • Inspisated mucus difficult to remove during bronchoscopy.
Classification of ABPA • ABPA with central bronchiectasis …..ABPA-CB • ABPA without bronchiectasis………….ABPA-S • ABPA with “other radiologic findings”..ABPA-ORF • ABPA is classified into 5 stages for ABPA-CB and 4 stages for ABPA-Seropositive • Patients can change stages over time in either direction except if stage 5 (end stage- fibrocavitary) Ricketti AJ, Greenberger PA et al Arch Int Med 1983; 143: 1553
Treatment Options • Oral Corticosteroids • Anti-fungals • Immunomodulators • TREAT the ASTHMA and CO-MORBIDITIES • CONSIDER ENVIRONMENTAL SOURCES Cochrane Review Wark PAB et al 2004
Prednisone as Monotherapy • 0.5mg/kg/each am for 2 weeks then on alterate mornings for 2 months….Tapered prednisone • Repeat HRCT examination • Repeat total IgE (should decline at least by 33%) • Environmental exposures to molds-inquire re home and workplace for obvious sources Ricketti AJ, Greenberger PA et al Arch Int Med 1983; 143: 1553 Cochrane Review Wark PAB et al 2004 ----
Antifungals • Oral (itraconazole, voriconazole, posaconazole) • Adverse effects of itraconazole… • gastrointestinal intolerance, • lfts, • headache, • peripheral neuropathy, • sleep disturbance….and • inhibition of cyp 3a4 dependent hepatic metabolism (increases concentration of prednisolone (not prednisone) and inhaled budesonide and fluticasone causing HPA suppression) Ricketti AJ, Greenberger PA et al Arch Int Med 1983; 143: 1553 Cochrane Review Wark PAB et al 2004 ----
53-year old nursePrednisone Plus Itraconazole • 0.5mg/kg/each am for 2 weeks then on alterate mornings for 2 months….Taperedprednisone • Plus Itraconazole400 mg daily for 16 weeks • Repeat HRCT examination • Repeat total IgE (should decline at least by 33%) • Environmental exposures to molds-inquire home and workplace for obvious sources
53-year old nurse - 4 months later • IgE=261 UI/l • Spirometry (basal): • FVC=82%, • FEV1=69%, • FEV1/FVC=68% • ACT score = 21; NO= 12 ppm • 4 MDIs (Ventolin) for one year • 1 exacerbation for one year Courtesy by Prof. Ruza Stevic
Omalizumab • Case reports (some +, some -) • Controlled trial for CF-ABPA initiated Thorax 2007;62:276-7.
Fungal sensitisation (Allergy SPT) is common in patients with life-threatening asthma in USA O'Hollaren et al New Engl J Med 1991; 324: 359Fungal sensitisation is common in patients with life-threatening asthma in New ZealandPoole PJ, Black PN Allergy 2000; 55: 501
Aspergillus 7% Candida 10% Penicillium 2% Cladosporium 1% (2%)* Alternaria 5% (4%)* Any Fungal Allergen 16% >1 Fungal Allergen 5% Aspergillus 37% Candida 33% Penicillium 30% Cladosporium 41% Alternaria 26% Any Fungal Allergen 76% >1 Fungal Allergen 50% Fungal sensitisation is common in patients with severe asthma in the UKNever Admitted n=82 >1 Hospital Admission n=46 * General European Adult PopulationSensitisation: Alternaria 4%, Cladosporium 2% Bousquet P et al. Clin Exp All 2007;37:780-87) O’Driscoll BR BMC Pulm Med. 2005 Feb 18;5(1):4.
ABPA Asthma (usually severe) Aspergillus sensitization(IgE) Eosinophilia Aspergillus sensitization (IgG) Very high IgE level Pulmonary Infiltrates Central bronchiectasis SAFS Severe Asthma Fungal sensitisation (IgE) Eosinophilia + / - The link between fungi and severe asthma: a summary of the evidence Denning DW et al. Eur Respir J 2006; 27:615-626
The Fungal Asthma Sensitization Trial (FAST) study • Atopy to fungal and non-fungal allergens is very common in severe asthma in North West England • SPT and RAST tests can identify fungal sensitisation • At present, it remains necessary to undertake both tests to identify all cases of fungal sensitisation • This may have therapeutic implications (ABPA and SAFS) Denning DW et al Am J Resp Crit Care Med 2008; In press
Asthma (and bronchiectasis) • Bronchiectasis (and asthma) Asthma Bronchiectasis