Download
1 / 2
20 likes | 121 Views
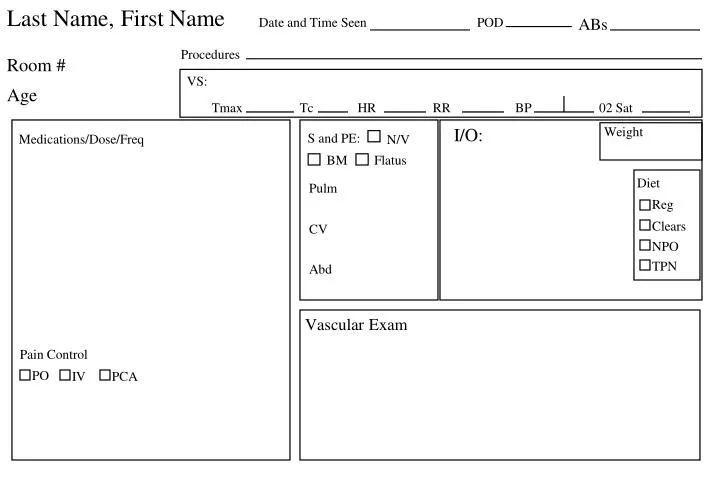
Last Name, First Name. Diet. Reg. Clears. NPO. TPN. Pain Control. PO. IV. PCA. ABs. Date and Time Seen. POD. Procedures. Room #. VS:. Age. Tmax. Tc. HR. RR. BP. 02 Sat. I/O:. Weight. S and PE:. Medications/Dose/Freq. N/V. BM. Flatus. Pulm. CV. Abd. Vascular Exam.

E N D
Last Name, First Name Diet Reg Clears NPO TPN Pain Control PO IV PCA ABs Date and Time Seen POD Procedures Room # VS: Age Tmax Tc HR RR BP 02 Sat I/O: Weight S and PE: Medications/Dose/Freq N/V BM Flatus Pulm CV Abd Vascular Exam
Last Name A/P and Orders: VS: Tmax Tc HR RR BP 02 Sat Date and Time PT LDH Bili AST PTT Amylase ALT INR Lipase GGT