Download
1 / 31
320 likes | 1.53k Views
Joint Hospital Surgical Grand Round 18 Apr 2009. Malignant Rectal Polyp. Dr Kit-wai Lai Department of Surgery Tuen Mun Hospital. Malignant Rectal Polyp. Polyps with cancer cells penetrating the muscularis mucosa Invasion limited to submucosa i.e. T1 lesion. >1cm 38.5% >42mm 78.9%.

E N D
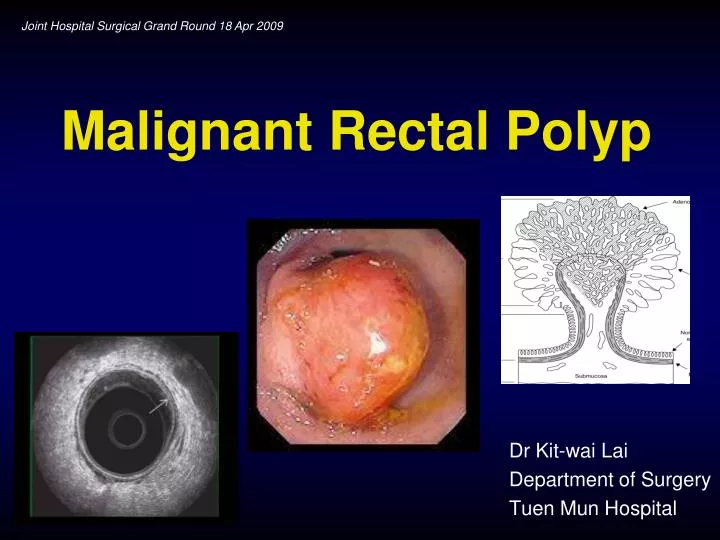
Joint Hospital Surgical Grand Round 18 Apr 2009 Malignant Rectal Polyp Dr Kit-wai Lai Department of Surgery Tuen Mun Hospital
Malignant Rectal Polyp • Polyps with cancer cells penetrating the muscularis mucosa • Invasion limited to submucosa • i.e. T1 lesion
>1cm 38.5% >42mm 78.9% Tytherleigh et al. BJS 2008;95:409-423 Malignant? Sizethe most important factor determining risk of malignant transformation within a polyp
Level 0: noninvasive (severe dysplasia) Level 1: invading through the muscularis mucosa but limited to the head of a pedunculated polyp Level 2: invading the neck of a pedunculated polyp Level 3: invading the stalk of a pedunculated polyp Level 4: invading into the submucosa below the stalk of a pedunculated polyp ( Sessile malignant polyplevel 4 ) Haggitt Classification
Kikuchi Classification of Adenocarcinoma in Sessile Polyp Haggitt level 1,2,3 = Kikuchi Sm1 level 4 = Sm1, Sm2 or Sm3
Local Therapy Opportunity of cure with less detriment Staging is critical to management Histological Assessment Most important factor to predict risk of lymphatic spread Tytherleigh et al. BJS 2008;95:409-423
Histopathological Features Best estimate of the probability of regional LN metastasis Bretagnol et al. Dis Colon Rectum 2007;50:523-533 Rate of lymph node metastasis Sm1 1-3% Sm2 8% Sm3 23% Nascimbeni et al. Dis Colon Rectum 2002;45:200-206 Poorly differentiated 43% Goldstein et al. Am J Clin Pathol 1999;111:51-8
2. Post Colonoscopic polypectomy of rectal polyp Pathology: adenocarcinoma arise from tubular adenoma Clinical Scenario • 1. • Colonoscopy: 2.5cm rectal polyp (3cm from anal verge) • Biopsy: adenocarcinoma
1. Colonoscopy: 2.5cm rectal polyp (3cm from anal verge) Biopsy: adenocarcinoma Clinical Scenario
LN - LN + T1 T2 Local Excision High Risks Features Sm3 (Sm2) Grade lymphovascular No High Risks Features Follow-up Local Excision + Adj ChemoRT Radical Sx AR/TME/APR Recurrence No Recurrence Salvage Surgery Scenario 12.5cm rectal Polyp Digital rectal exam ERUS MRI CT
ERUS • Best method to determining Tstage Bretagnol et al. Dis Colon Rectum 2007;50:523-533
ERUS • T1-slight (Sm1) detection Sensitivity (99%) Specificity (74%) Accuracy (96%) Akasu et al. World J Surg 2000;24:1061-1068 • May assess residual tumour following polypectomy • Follow up after local excision or radical surgery Hernandez De Andaetal. Dis Colon Rectum 2004; 47: 818–824 • Limitations Sm1 • Operator dependent • Tumor height • Tumour stenosis • Peritumoral fibrosis and inflammatory tissue • Effect of pre op radiotherapy or haemorrhage in bowel wall after bx Sm2
MRI • Overall T stage accuracy 59-95% • T1,2 lesion (vs ERUS) • Similar sensitivities • Lower specificity (69%) • N stage • Comparable vs ERUS Bretagnol et al. Dis Colon Rectum 2007;50:523-533
Scenario 12.5cm rectal Polyp Digital rectal exam ERUS MRI CT LN - LN + T1 T2 Local Excision High Risks Features Sm3 (Sm2) Grade lymphovascular No High Risks Features Follow-up Local Excision + Adj ChemoRT Radical Sx AR/TME/APR Recurrence No Recurrence Salvage Surgery
Local Excision • Potential advantage • Sphincter preservation • Minimal mortality and morbidity • Low urinary/sexual dysfunction risk
Local Excision • Parks’ Per Anal Excision • Lesions 6-10cm from anal verge • Aid of anal retractors • Full thickness excision • Transanal Endoscopic Microsurgery • Resectoscope • Usual below peritoneal reflection • Full thickness excision
Local Excision LR Bretagnol et al. Dis Colon Rectum 2007;50:523-533
Local Excision vs Radical Sx T1sm3 lesion Radical Surgery had lower rates of distant metastasis and better survival Bretagnol et al. Dis Colon Rectum 2007;50:523-533
Scenario 12.5cm rectal Polyp Digital rectal exam ERUS MRI CT LN - LN + T1 T2 Local Excision High Risks Features Sm3 (Sm2) Grade lymphovascular No High Risks Features Follow-up Local Excision + Adj ChemoRT Radical Sx AR/TME/APR Recurrence No Recurrence Salvage Surgery
Adjuvant chemoradiotherapy • Limited data • May be helpful If further surgery is not an option T1 lesions with adverse pathologic features T2 lesions (Tytherleigh et al. BJS 2008;95:409-423) Difficult to interpret Most retrospective studies Lack of controlled data Adjuvant regime not always based on a defined protocol Bretagnol et al. Dis Colon Rectum 2007;50:523-533
Scenario 12.5cm rectal Polyp Digital rectal exam ERUS MRI CT LN - LN + T1 T2 Local Excision High Risks Features Sm3 (Sm2) Grade lymphovascular No High Risks Features Follow-up Local Excision + Adj ChemoRT Radical Sx AR/TME/APR Recurrence No Recurrence Salvage Surgery
Follow up • Regular endoscopic surveillance of rectum and scar • Digital rectal exam + Endoscopy + CEA • First 2 years: every 3 months • Next 3 years: every 6 months • Then annually Mellgren et al. Dis Colon Rectum 2000; 43: 1064–1071 NCCN guideline
Follow up • ERUS • Advisable • Frequency: subject to debate • One study showed Moreisolated local recurrence in the follow-up ERUS group underwent SalvageSurgery (44% vs 23 %), but the differences were not significant Hernandez De Andaetal. Dis Colon Rectum 2004; 47: 818–824
Scenario 12.5cm rectal Polyp Digital rectal exam ERUS MRI CT LN - LN + T1 T2 Local Excision High Risks Features Sm3 (Sm2) Grade lymphovascular No High Risks Features Follow-up Local Excision + Adj ChemoRT Radical Sx AR/TME/APR Recurrence No Recurrence Salvage Surgery
Recurrence • Long-term FU beyond 10 years is necessary • Unresected disease in regional lymphatics cause local failure • Diagnose early for salvage surgery Tytherleigh et al. BJS 2008;95:409-423
Salvage Surgery • 56-100% of patients with recurrence suitable for salvage surgery • Results controversial • May not afford same outcomes as initial classical treatment • Decreased survival if resection is delayed at time of recurrence (for adverse pathology of local excision specimen) Mellgren et al. Dis Colon Rectum 2000; 43: 1064–1071
2. Colonoscopic polypectomy of rectal polyp Pathology: adenocarcinoma arise from tubular adenoma Clinical Scenario
Scenario 2 Post polypectomy (Adenoca arise from TA) No High Risks Features Haggitt level 1,2,3 Kikuchi Sm1 High Risks Features Sm3 (Sm2) Grade lymphovascular ERUS MRI CT LN- LN+ Margin involvement Yes Histological assessment not adequate No Local Excision No Yes Follow up Radical Surgery High Risks Features
Summary Stagingand Adequate HistologicalAssessment is crucial in management of malignant rectal polyp
Summary • Local excision Recommended for low risk T1 sm1 lesion • Adjuvant therapy considered in high risk T1, T2 if surgery not an option • Radical Surgery Recommended for high risk T1 , T2 lesion • Recurrence Diagnose early for salvage surgery