Download
1 / 28
290 likes | 580 Views
Valve Replacement in Infective Endocarditis. PJA Slabbert Cardiology. Patient history. 34 year male from NC Admitted KHC : 23/3/10 to 8/4/10 for Infective Endocarditis (culture negative) Pen G and Gentamycin Clinically deteriorated over 3 days and follow up echocardiogram showed:

E N D
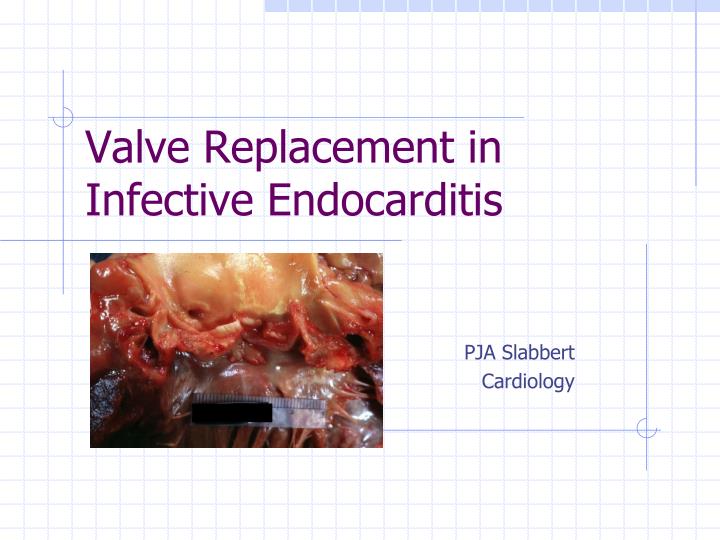
Valve Replacement in Infective Endocarditis PJA Slabbert Cardiology
Patient history • 34 year male from NC • Admitted KHC : 23/3/10 to 8/4/10 for Infective Endocarditis (culture negative) • Pen G and Gentamycin • Clinically deteriorated over 3 days and follow up echocardiogram showed: • Worsening heart failure • More extensive vegetations on aorta valves
Systemic enquiry: • Neurology: no TIA, no amurosis fugax • Respiratory: 3 weeks non productive cough, progressive dyspnoea • Cardiology: Angina on exertion, ortopnea, PND, dyspnoea NYHA grade 4, ankle swelling, no sharp chest pain radiating to back. • Gastro-enterology: vomited previous night. • Previous medical Hx: • D-E-A-T-H-, not known with cardiac condition, no chronic medication
Examination • General: • Chronically ill: underweight • J-A-C-C-O+L- • BP 121/52 (no cardiogenic shock, wide pulse pressure), HR 92/m, normal temperature, RR 33/m, saturation 98% on 40% oxygen • Diffuse fungal/ yeast skin infection: • Pityriasis versicolor • No peripheral manifestations of infective endocarditis: Roth spots, subungual hemorrhages, Janeway lesions
Cardiovascular • Water hammer pulse, equal pulses and BP left and right. Elevated JVP 2cm above baseline • Apex displaced inferior lateral: 6th ics aal • Loud P2, C3 both ventricles • Decrescendo diastolic murmur parasternally with ejection systolic murmur not radiating. No Austin Flint
Respiratory: • Diffuse inspiratory crackles • Distressed : tachypnoea, accessory muscle use. • Abdomen: • No Hepatomegaly, No splenomegaly • Urine Dipstix : • no microscopic hematuria
Problem List • Infective Endocarditis • Severe Aorta Regurgitation with signs of bi-ventricular failure • Pulmonary edema with acute respiratory failure
Special investigation • Bloods: • FBC : WCC 8.4, Hb 14.1, plt 191 • U&E : Na 136, K 5.2, Urea 17.6, Cr 133 • LFT : t-prot 72, alb 25, t-Billi 35, c-Billi 16, ALP 109, GGT 108, AST 165, ALT 293, LDH 150 • CRP 5.2 • Trop-T : negative, CK : normal • ASOT negative, ANA negative, RF negative, RPR negative, HIV negative • BC negative • Cardiac echo • CXR • ECG
echo • Aorta root diameter = 30 mm (normal) • Aorta valve opening = 21 mm (normal) • Vegetation on all three aorta cusps • Pressure half time = 67 ms (<200ms severe acute AR) • Mitral valve : mild regurgitation • Left Atrium : 4.3 cm (enlarged) • Left ventricle: LVEDD 6.5 cm, LVESD 5 cm, LVEF = 44% • Right heart mildly enlarged, mild TI, RVPSP = 65 mmHg
Treatment • Furosemide 40 mg bd ivi • Enalapril 5 mg bd po • Elantin 20 mg bd po • Pen G, Gentamycin, Cloxacillin, Diflucan • Urgent cardio-thoracic consult • Ross procedure was done
Surgery in NVE • Introduction • 1961 : Kay and colleagues excised fungal vegetation from tricuspid valve • 1965 : AVR in IE due to Serratia Marcescens • Last 3 decades : valve replacement/ repair common in Mx of complicated IE • Decreased mortality in IE due to combination of antibiotics and timely surgical intervention
Indications • 2006 American College of Cardiology/ American Heart Association (ACC/ AHA) • Surgery is warranted for native valve IE who have one or more of the following • 1. Heart failure (moderate to severe) that is directly related to valve dysfunction. • 2. Severe aorta/ mitral regurgitation with evidence of abnormal hemodinamics, such as elevated LVED or left atrial pressures. • 3. Endocarditis due to fungal of high resistant organisms. • 4. Peri-valvular infection with abscess/ fistula formation
Other condition considered as possible indications • 1. Embolic events while on appropriate antibiotic regimen or large vegetations (> 10mm in diameter) • 2. Large vegetations > 10mm in diameter (even without embolic events) if mobile
Choice of procedure • For active infection (2006 ACC/AHA): • Valve repair rather than replacement • Only possible in minority of cases • Thus leaflet perforation without destruction or annular involvement.
Heart Failure • Moderate to severe HF due to IE • Medical therapy : mortality rate 75% • Medical & surgical : mortality rate 25% • HF is indication in 2/3 to ¾ of cases • IE induced AR is more likely to produce HF than IE induced MR (death may occur suddenly in aorta involvement)
Caveats • Non cardiac factors that exaggerate HF • Fever, anemia, sepsis, renal insufficiency • Hx of previous HF. • HF out of proportion to valve dysfunction.
Complicated infection • Persistent positive BC • 5 to 7 days or lack of clinical improvement after 1 week of appropriate Rx search for metastatic abscess; then • Echocardiographic evidence of perivalvular abcess / fistula formation/ leaflet perforation • Serial TEE and early in presence of known difficult organism. • New heart block
Fungal infection is in general an early indication for • Relapse after adequate therapy may require intervention. A 2nd course of antibiotics is only indicated if no perivalvular infection and offending organism is sensitive to Rx.
Embolization • Overall risk : 13 – 44% • Decline after effective antimicrobial Rx, thus not necessary to prevent stroke. • indicated after a second embolic event after appropriate Rx in patient with persistent vegetations. • ‘Silent’ emboli, thus screen (CT scan) all patient with large (>1cm) or mobile vegetations prior to
Emboli ( risk) • Cardiopulmonary bypass and need for anticoagulation increases the risk of extending infarct and or converting a nonhemorrhagic infarct into a hemorrhagic lesion. • Suggested is postponed 2 weeks after cerebral infarction and 4 weeks after cerebral hemorrhage. • May be done before 2 weeks if compelling indications (eg moderate HF).
Emboli (vegetation size) • Larger size larger risk for emboli • In general is not indicated for increase in vegetation size in patient responding well to medical Rx • Vegetations > 10mm by itself is not sufficient to require , unless other complicating features.
Timing of surgery • Concern: placing prosthetic valve in actively infected tissue ! • Recommendation: should not be delayed with clear indications regardless of duration of pre-operative antibiotics.
Antibiotic following surgery • 2004 European Society of Cardiology (ESC): • Full course of antibiotic Rx if valve culture is positive • If culture negative, complete full course counting the pre-operative duration of Rx. Minimum duration 7 to 15 days post operative. Rate of relapse 3/358
Reference • Fauci, AS, Braunwald, E, Harrison’s Principles of Internal Medicine, 17th Edition, 2008 • Schick, EC, Surgery for native valve endocarditis, Uptodate, June 2008 • Talley, NJ, O’Conner, S, Clinical examination, 2001
Q & A • Thank you






















