Download
1 / 28
300 likes | 666 Views
Blood groups and Hemostasis. Dpt. Of Normal, Pathological and Clinical Physiology. Blood groups. blood transfusion often resulted in agglutination and hemolysis , often led to death (renal shock)

E N D
Blood groups and Hemostasis Dpt. Of Normal, Pathological and Clinical Physiology
Blood groups • blood transfusion often resulted in agglutination and hemolysis, often led to death (renal shock) • antibodies in the plasma of one blood react with antigens on the surface of the red cells of another blood • more than 30 commonly occurring antigens • hundreds of rare antigens • two particular groups of antigens: AB0 and Rh systems are immunogenic enough to cause hemagglutination
Landsteiner Jánský actual nomenclature A II A B III B C I 0 --- IV AB AB0 system - history
AB0 system • four groups: A, B, AB, 0 • two (3) agglutinogens = antigens on the surface of RBC • two agglutinins = antibodies present in the plasma • agglutinogens = glycoprotein, oligosaccharides having different carbohydrate at their endings A – N-acetylgalactosamin B – galactose H – fucosotransferasa
AB0 agglutinogens • determined by two genes, one on each of two paired chromosomes • 0 is functionless gene; O = “ohne” • A gene determines A group; B gene determines B group • codominancy: • blood type A: genotype AA, A0 • blood type B: genotype BB, B0 • blood type AB: genotype AB • blood type 0: genotype 00 (or hh “Bombay” + either AA, AO, BB, BO, or AB) + Hh or HH
AB0 agglutinogens • antigen H forms the antigen-carrying molecule • subtypes of A antigen A1…A6, different immunogenity • detectable in 4weeks old embryo • during labor, 20-30% of the immunogenity in adult (> 18 years)
AB0 agglutinins • antibodies present in the plasma • γ-globulins, IgGand IgM molecules (pentamers, not diffusing trough the placenta) • not present immediately after birth • produced in 2-8 months after birth by plasma cells (specialized B-cells, stimulated by similar oligosaccharides often expressed in the nature – food, intestinal bacterias) • highest titer around at 10 years of age • antibodies against the AB0type not present in the blood • group A antibodies anti-B • group B antibodies anti-A • group AB no antibodies • group 0 antibodies anti-A and anti-B
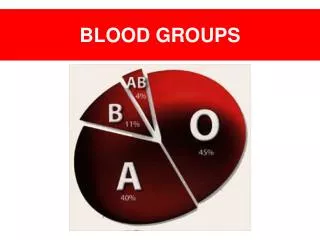
Frequencies of the different blood types • differ according to geographic and time locations • group A: Atlantic population and Eskimos (60%) • group B: east-south Asia, India (40%) • group 0: America'sIndians (100%) • the Czech Rep.: A-42 %, 0-32 %, B-18 %, AB-8 % • white people: A-47 %, 0-41 %, B-9 %, AB-3 % • universal donor, universal acceptor - antigens • autotransfusion
Rh system II • Landsteiner 1940 • C, D, E antigens (D is most immunogenic) • 85 % white people Rh+, 99 % Asians Rh+, African black 100 % Rh+ • clinical importance: • blood transfusion • pregnancy: mother Rh negative and fetus Rh positive, antibodies diffuse trough the placenta (erythroblastosis fetalis, new-born hemolysis, kernicterus, jaundice) in both cases the exposition to the antigen is needed first (sensitization), because anti-Rh antibodies are NOT normally produced – Rh antigen is not often present in the nature
Other systems • MNSs: very low immunogens, normally no natural antibodies in blood occur, Landsteiner 1927 • P system: Landsteiner, low immunogens ( 80% people); subtypes • Kell, Duffy, Kidd, Lutheran, Diego
Hemostasis • three mechanisms: • vascular spasm • formation of a platelet plug • blood coagulation
Vasoconstriction • neural: nervous reflexes induces by activation of pain fibers, local myogenic spasm • humoral: thromboxan A2andserotoninand other substances produced by activated platelets • vasoconstriction itself stops the bleeding in vessels as large as a. radialis (under ideal circumstances / i.e. crushed, not cut) • lasts for minutes or even hours
Platelets • do not have nuclei, oval discs 2-4 mm, half-life 4-8days • megakaryocytes (1000-5000 platelets) • 150 – 300.000 per 1 microliter • platelets cytoplasm contains: • actin and myosin and thrombosthenin (platelet contraction) • vesicles containing Ca2+ , serotonin, ADP • enzymes that synthesize prostaglandins • a-granules: PDGF, coagulating factors, von Willebrandt factor (adhesion) • lysozomy • platelets membrane contains large amount of phospholipids
platelets function • adhesion, collagen: vonWillebrandt Factor released from endothel • activation: swelling, irregular forms, pseudopods, release of serotonin, vWF, tromboxan A2, ADP activation of other platletes • aggregation: stimulated by trombin, tromboxan A2, vWF, fibrinogen platelet plug (loose, then fibrin threads form an unyielding plug) closing the minute ruptures (small vessels, many times per day, petechiae)
Thrombopoetin • produced bythe liver,little in kidney • receptors in plasma membrane of stem cells and megakaryocytes andplatelets (regulation) • constant production, regulation by the number of platelets / the more platelets the more T bound to them less T act on stem cells and megakaryocytes • liver diseases bleeding (together with lower production of clotting factors)
clotting pathways • the sense is to form fibrinmonomers and then polymers = fibrin fibers (threads) within few seconds (and pesence of Ca2+) • fibrin is formed by activated thrombin all activators of prothrombin are called trombokinases (tissue and plasmatic trk) intrinsicpathway extrinsic pathway common
clotting factors - proenzymes * vitamin K dependent
clotting pathway – common X Þ Xa: activated either by intrisic or extrinsic pathway II Þ IIa: protrombin, trombin XIII Þ XIIIa I Þ Ia:fibrinogenfibrin +V stabilization
clotting pathway – intrinsicsubmucosis, phospholipids released from platelets XII Þ XIIa: catalyzed by kalikrein a kininogen, activated by negative charges (glass, collagen) XI Þ XIa: activated by XIIa IX Þ IXa: activated byXIa X Þ Xa 1 – 6 minutes +VIII
clotting pathway – extrinsictissue, lipoproteins VII Þ VIIa: activated by tissue factor III(thromboplastin) which is released from damaged tissues X Þ Xa: activated byVIIa 10 seconds, explosive (VIIaactivatesIXof intrinsic pathway as well)
anticlotting mechanisms • endothelial smoothness, glycocalyx (mucopolysaccharide repelling the factors) and thrombomodulin (protein binding thrombin) • fibrin itself remove thrombin from the blood • catching of activated factors by liver • consumption of activated factors • antithrombin III: proteases inhibitor, its binding is facilitated by heparin no activation of IX, X, XI, XII • heparin – polysaccharide released from mast cells and basophils
fibrinolysis • thrombomodulin (endotelial wall) catalyzesactivation of protein C by thrombin • activated protein C (APC) • inactivates VIII • inactivates V • activates tissue plasminogen activator (TPA) • TPA catalyzesactivation of plasminogen to form plasmin, plasmin causes lysis of the clot • alteplase (recombinant), streptokinase, urokinase
anticoagulants • heparin (+ antithrombin III) • citrate, oxalate (bind Ca2+) • coumarin, warfarin (inhibition of vitamin K)
excessive bleeding • failure of blood clotting (coagulopathy) • hematoms, joint bleeding • platelets failure thrombocytopathy • petechiae • vessels defects • petechiae
innate coagulopathy • abnormality or deficiency of one of the clotting factors • hemophilia A, classic h. • defect of VIII (3 subunits, defect of the clotting factor) • transmitted genetically, X chromosome, males • hemophilic arthropathy, muscle bleeding in legs • 1 z 10000 born males • von Willebrandt disease: defect of VIII, all subunits impaired (vW factor, antigen factor and clotting factor) • hemophilia B: defect of IX • other disorders when impaired factors I, II, V, VII, X, XIII • deficiency of XI almost without any clinical signs
acquired coagulopthies • liver diseases (cirrhosis) – deficiency of all factors • heparin • deficiency of vitamin K • DIC • sepsis, leukemia, AB0 incompatibility
defects of platelets • trombocytopenia: aplasia (radiation), hypovitaminosis B12, sequestration • trombocytopathy: acetylsalicylic acid (inhibition of COX Þ suppresses synthesis of thromboxan A2 and secretion of ADP
Defekty cév • von Willebrandtova choroba: defekt endotelu, chybí vWF Þ porucha adheze, nedostatek VIII (vWF je jeho přenašeč) • skorbut • vrozené defekty pojiva: Rendu-Osler, Henoch-Schönlein