Download
1 / 19
190 likes | 328 Views
Dying to be Thin: A Discussion of Eating Disorders. Pamela S. Chally, PhD, RN Dean/Professor. University of North Florida College of Health 4567 St. Johns Bluff Rd. S Jacksonville, Florida 32224 pchally@unf.edu. Shocking Facts About Eating Disorders.

E N D
Dying to be Thin: A Discussion of Eating Disorders Pamela S. Chally, PhD, RN Dean/Professor University of North Florida College of Health 4567 St. Johns Bluff Rd. S Jacksonville, Florida 32224 pchally@unf.edu
Shocking Facts About Eating Disorders • An estimated 8,000,000 people suffer from eating disorders in the United States. • An estimated 3-6% of the serious cases will die - - a far higher death rate than for any other mental illness. • Although most anorexics or bulimics start in their teens, victims range from five years to seventy years old. • The number of males and people of color suffering from eating disorders is increasing.
WARNING SIGNS!! of Anorexia-self imposed starvation • Deliberate self starvation • Intense fear of gaining weight • Plans and cooks elaborate meals • Refusal to eat, except for tiny portions • Denial of hunger • Compulsive exercise
WARNING SIGNS!! of Anorexia-self imposed starvation • Distorted body image • Cold intolerance • Absent menstruation (primary & secondary) • Hair loss and/or fine, downy hair on body • Wears loose, baggy clothing • Dizziness and headaches
WARNING SIGNS!!of Bulimia-repeated cycle of out-of-control eating followed by purging • Binge eating, usually in secret • Preoccupation with food • Vomiting after bingeing • Frequent use of the bathroom after meals • Abuse of laxatives, including diuretics, diet pills, or emetics
WARNING SIGNS!!of Bulimia-repeated cycle of out-of-control eating followed by purging • Weight fluctuations • Swollen salivary glands • Broken blood vessels in eyes and/or mini bruises on face • Bruised or callused knuckles • Feeling guilty about eating • Feeling out of control • Dental caries
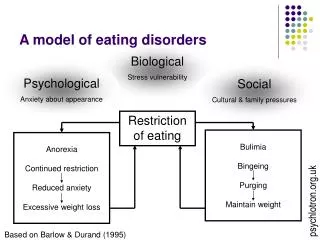
Biological Psychological Family Sociocultural Abnormal attitude toward weight and shape PREDISPOSINGFACTORS PRECIPITATINGFACTORS PERPETUATINGFACTORS BINGE AND/ORPURGE CYCLE STRESSORS Extreme Behavior Physiological andPsychologicalResponses OvereatingorExtreme dieting
Medical Complications of Eating Disorders Short Term: • Osteoporosis • Slow heart beat • Dehydration • Cold intolerance • Tooth and gum erosion • Inflammation or ulcers of the stomach or esophagus • Amenorrhea or menstrual irregularities • Low blood pressure (anorexia) • High blood pressure (compulsive overeating)
Medical Complications of Eating Disorders Long Term: • Infertility • Renal disease • Liver damage • Electrolyte imbalance • Seizures • Cardiac arrhythmias • Death
PsychologicalComplications of EatingDisorders • Low self-esteem • Body image disturbance • Inability to concentrate • Depression • Obsessive-compulsive disorders • Bi-polar disorders • Attention deficit disorders
Social Consequences of Eating Disorders • Unrealistic representation of the perfect body continues • Unhealthy relationships • Social isolation • Treatment costs • Work absences • Lost of potential of 5-10% of the female population
Risk Factors • Female, middle or upper social class • Family history of eating disorder, depression, or obsessive compulsive disorder • Overly compliant • Desires to be in control • Overachiever, perfectionist • Compulsive
Risk Factors • Denies feelings • Low self esteem • Is or has been dieting • Has trouble with close relationships • Participates in body conscious sports or activities • Recent family crisis
Case Study: Anorexia Nervosa Jane is a 13-year-old whose grades have been excellent andwhom the teachers describe as a “model student.”Recently some of Jane’s friends have expressed concern tothe school nurse practitioner that Jane has begun to “jog” atlunch time and seldom eats with them.Jane has told her friends that she has gained weight over thewinter months and that she is “jogging” because she wants to qualify for the track team this spring.
The Anorexic ClientNursing Care Plan Nursing Diagnosis:Imbalanced nutrition: less than body requirements related to self-starvation. Goal 1: Will consume nourishment adequate for weight gain Goal 2:Will follow behavior-modification plan (if implemented) Goal 3:Will reduce energy expenditure
The Anorexic ClientNursing Care Plan Nursing Diagnosis:Disturbed body image related to altered perception Goal 1: Will express self in acceptable ways Goal 2:Will receive adequate support Goal 3:Will receive assistance in altering distorted self-image
The Anorexic ClientNursing Care Plan Nursing Diagnosis:Ineffective coping related to unrealistic perceptions Goal 1: Will conform to therapeutic program Nursing Diagnosis:Readiness for enhanced family coping related to ambivalent family relationship Goal 1: Will recognize disturbed pattern of family interaction (if applicable)
Recommended Treatment of Eating Disorders • Regular physical monitoring by a medical doctor who understands eating disorders • Individual therapy • Group therapy • Family therapy • Marital therapy
Recommended Treatment of Eating Disorders • Support groups • Nutritional counseling • Special outpatient therapy programs • Hospitalization for physical stabilization and concentrated focus on behavioral and emotional growth