Download
1 / 109
1.12k likes | 1.17k Views
DISEASES OF THE BLOOD VESSELS. ATHEROSCLEROSIS. Dr Eman MS Muhammad. DISEASES OF THE BLOOD VESSELS. Diseases of arteries Degenerative Inflammatory Obliterative Aneurysms Diseases of veins. Normal structure of the blood vessels: The wall of the arteries is composed of three coats:

E N D
DISEASES OF THE BLOOD VESSELS ATHEROSCLEROSIS Dr Eman MS Muhammad
DISEASES OF THE BLOOD VESSELS • Diseases of arteries • Degenerative • Inflammatory • Obliterative • Aneurysms • Diseases of veins
Normal structure of the blood vessels: • The wall of the arteries is composed of three coats: • The intima: The inner most layer. • It consists of endothelium. • It is separated from the internal elastic lamina by loose connective tissue (CT). • The media:consists of tight spiral of smooth muscles which lie in a meshwork of elastic and collagen fibers.
The amount of stroma increases with increased vessel size. • An external elastic lamina separates the media from the adventitia. • The adventitia:is composed of a thin layer of loosely arranged collagen and elastic fibers. • It is rich in lymphatics and traversed by nerves.
All layers of the smallest arteries are supplied with oxygen and nutrition by diffusion from the lumen. • Large arteries have small vessels; the vasavasorum, which supply the adventitia and outer part of the media. • While the inner part of the wall depends on diffusion from the lumen for its nourishment. • The differences in the structure of the media of arteries of various sizes are reflected in their functions. • The large elastic arteries absorb part of the force of left ventricular systole and their recoil helps to sustain the pressure for continued blood flow during diastole.
The smaller arteries and arterioles; resistance arterioles, regulate the overall arterial pressure and blood flow to the individual organs and tissues. • These functions reflected on the predominance of smooth muscles in the media. • The smooth muscles has rich autonomic innervations, which with the circulating levels of vaso-active hormones and factors produced by the endothelial cells, controls the caliber. • The smooth muscles of the media are not only contractile, but they also synthesize the matrix protein of the artery; collagen, protein and proteoglycan.
The endothelium regulates the activity of platelets. • It has an important role in modulating both coagulation and fibrinolytic system. • The endothelium also directly regulates vascular tone by secreting the vasodilator endothelial derived relaxant factor EDRF. • The action of EDRF is counterbalanced by the secretion of the vasoconstrictor peptide endothelin, the most potent vasoconstictor known.
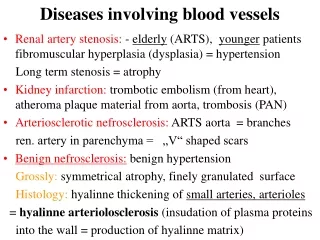
Diseases of Arteries • Arteriosclerosis: • Atherosclerosis • Monkeberg’s medial calcific sclerosis • Arteriolosclerosis • Inflammations (arteritis- vasculitis or vasculitides), polyarteritisnodosa (PNA), Buerger’s disease, giant cell arteritis, Wegener’s granulomatosis, ……etc • Aneurysms.
Terminology • The following terms are similar, yet distinct, in both spelling and meaning, and can be easily confused: arteriosclerosis, arteriolosclerosis, and atherosclerosis. • Arteriosclerosisis a general term describing any hardening (and loss of elasticity) of medium or large arteries. • Arteriolosclerosisis any hardening (and loss of elasticity) of arterioles (small arteries).
Atherosclerosisis a hardening of an artery specifically due to an atheromatous plaque. • Atherogenic is used for substances or processes that cause atherosclerosis.
Atherosclerosis (Atheroma) • Definition: Atherosclerosis (AS)is acommon degenerative disease in which patchy deposits of fatty material develop in the walls of medium-sized and large arteries, followed by fibrosis, leading to reduced or blocked blood flow. • It is a slow complex disease in which fatty substances, cholesterol, cellular waste products, calcium, and other substances build up in the inner lining of an artery.
This buildup is called plaque. • AS is derived from the Greek words athero (meaning gruel or paste) and sclerosis (meaning hardness). • Recently, atherosclerosis is defined as a chronic multifocal immuno-inflammatoryfibroproliferative disease affecting large and middle-sized arteries, mainly induced by lipids accumulation.
General consideration: • In most developed countries atheroma is responsible for more deaths than any other diseases. • It is the main cause of disability and death from heart diseases, cerebral infarction and of ischemia of the lower limbs and gut. • It is always present in some degree in middle-aged and old people in most industrialized Western countries.
It causes narrowing of the lumen of the arteries. • The lesions of atheroma consist of patches “plaques” of intimal thickening of arteries. • This is due to accumulation of lipids, proliferation of smooth muscle cells, and formation of fibrous tissue. • It is often complicated by occlusive thrombosis.
The term AS is used because the lesion has a soft lipid-rich part “athere” and a hard “sclerotic” fibrous component. • The short term atheroma has historical priority and is less easily confused with the quite separate process of arteriolosclerosis (hypertension).
Macroscopic picture: • The earliest deposits of lipids in the intima of the aorta and large arteries occur predominantly in childhood and adolescence. • They are known as “fatty streaks”. • They appear as yellow slightly raised areas on the luminal surface, which enlarge and coalesce to form irregular yellow streaks.
They consist of accumulation of lipid droplets beneath the endothelium, both free and as aggregates within the macrophages. • Other lesions which may precede atheroma include: • Foci of intimal edema, and ↑ in the ground substance known as gelatinous patches, and some intimal thickening composed of smooth muscle cells, collagen and other extra cellular proteins “intimal cushions” which occur at the branching points of the arteries.
Small disc like slightly raised patches “plaques”of intimal thickening with smooth glistening surface. • The patches enlarge and thicken by further deposition of lipids deep in the intima and by fibrosis more superficially. • When viewed from the intimal surface these raised plaques appear yellow or white depending on the amount of fibrous tissue overlying the lipid deposits.
The patches vary in thickness, reflecting their development and slow growth throughout life.
Microscopic picture: • The earliest changes are due to the proliferation of smooth muscle cells in the intima and the accumulation of lipids in “foam cells”. • Some foam cells are macrophages; derived from monocytes which adhere to and then penetrate the endothelium. • Others are medial smooth muscles which proliferate and migrate into the intima. • Both absorb lipids and their cytoplasm becomes swollen with lipid globules.
Extra-cellular lipids accumulate in the intima near to the media in relation to elastic fibers and the internal elastic lamina. • As the patches develop, thin strands of CT appear sub-endothelially and between the foam cells and form the fibrous part of the lesion “fibrous cap”. • Areas of necrosis develop in the deeper part of the lesion converting it into a structureless accumulation of extracellular lipids, cholesterol crystals and tissue debris.
Infiltration by PNL and other inflammatory cells is common. • The internal elastic lamina is disrupted. • Necrosis and fibrosis then erode into the adjacent media. • As the plaques thicken, the underlying media becomes thin and atrophic.
Small blood vessels grow into the atheromatous plaque from the vasavasorum and from the lumen of these vessels. • They may hemorrhage contributing altered blood constituents to the plaque contents. • Some plaques may crack and rupture causing hemorrhage into the plaque leading to the formation of thrombus.
Clinical effects: • They vary depending on the size of the artery involved: • Uncomplicated atheroma of large arteries usually has no clinical effectsbecause it doesn’t reduce the lumen significantly or seriously thicken the wall. • In advanced cases an aneurysm may form. • Mural thrombus seldom causes complete occlusion of the aorta except at or near its bifurcation, with resulting coldness and weakness of the legs, muscle wasting, and sexual impotence.
Fragments of thrombi and athermanous debris from ulcerated plaques may form emboli which lodge in arteries of the legs and abdominal organs such as the gut, kidneys and spleen. • The most important effect of atheroma is due to involvement of smaller arteries. • The lumen may be progressively narrowed by an atheromatous plaque causing chronic ischemia or suddenly occluded by thrombosis which often causes infarction.
In smaller arteries, thrombosis is often precipitated by a crack in the fibrous cap rather than complete ulceration of the plaque. • The most dangerous effect is the coronary artery thrombosis. • Atheroma is the chief cause of ischemic heart disease, the largest single cause of death in developed countries. • Atheroma also is a very common cause of cerebrovascular diseases, due to atheroma of the carotid, vertebral and cerebral arteries.
Aneurysm may develop in the circle of Willis. • Peripheral vascular diseaseis also common especially in diabetics, and cigarette smokers. • Intermittent claudication painproduced in the leg due to muscle ischemia induced by exercise and relieved by rest. • If ischemia is severe gangrene may develops which starts in the toes and spreads proximally.
Clinical complication of atheroma: • Ischemic heart diseases: • Sudden death • Angina pectoris • Myocardial infarction • Cardiac arrhythmias • Cardiac failure
Cerebral ischemia • Transient cerebral ischemic attack • Dementia • Cerebral infarction • Mesenteric ischemia • Abdominal claudication • Malabsorption syndrome • Bowel infarction
Peripheral vascular disease • Intermittent claudication pain • Gangrene • Renovascularhypertention • Renal artery stenosis • Aneurysms • Aorta • Iliac and popliteal arteries • Cerebral arteries specially “Circle of Willis”
Atheroma& Lipid Metabolism • Lipid in the blood is carried on lipoproteins • Lipoproteins carry cholesterol and triglycerides (TG) • Hydrophobic lipid core • Hydrophilic outer layer of phospholipid and apolipoprotein (A-E)
Atheroma& Lipid Metabolism • Chylomicrons • Transport lipid from intestine to liver • VLDL • Carry cholesterol and TG from liver • TG removed leaving LDL • LDL • Rich in cholesterol • Carry cholesterol to non-liver cells • HDL • Carry cholesterol from periphery back to liver
Lipids circulate in plasma in combination with proteins in the form of lipoproteins. • Type of lipoprotein Type of lipid • Chylomicrons………. Triglycerides (90%) • HDL………….. Cholesterol (<20%) • LDL…………... Cholesterol (75%) • VLDL…………. Cholesterol (25%)
Atheroma& Apolipoprotein E • Genetic variations in Apo E are associated with changes in LDL levels. • Polymorphisms of the genes involved lead to at least 6 Apo E phenotypes. • Polymorphisms can be used as risk markers for atheroma.
Familial Hyperlipidemia • Genetically determined abnormalities of lipoproteins. • Lead to early development of atheroma. • Associated physical signs: • tendon xanthomas • xanthelasma
Xanthelasmais a sharply demarcated yellowish deposit of fat underneath the skin, usually on or around the eyelids. • They are neither harmful nor painful. • These minor growths may be disfiguring and can be removed. • A xanthelasma may instead be referred to as a xanthoma when becoming larger and nodular, assuming tumorous proportions. • Still, xanthelasma is often classified simply as a subtype of xanthoma.
A xanthoma (pleural, xanthomas or xanthomata) (condition: xanthomatosis), from Greek (xanthos), meaning 'yellow', is a deposition of yellowish cholesterol-rich material that can appear anywhere in the body in various disease states. • They are cutaneous manifestations of lipidosis in which lipids accumulate in large foam cells within the skin. • They are associated with hyperlipidemias, both primary and secondary types.