Download
1 / 1
10 likes | 179 Views
Towards Early Biochemical Screening for Fetal Aneuploidy in the First Trimester. Results

E N D
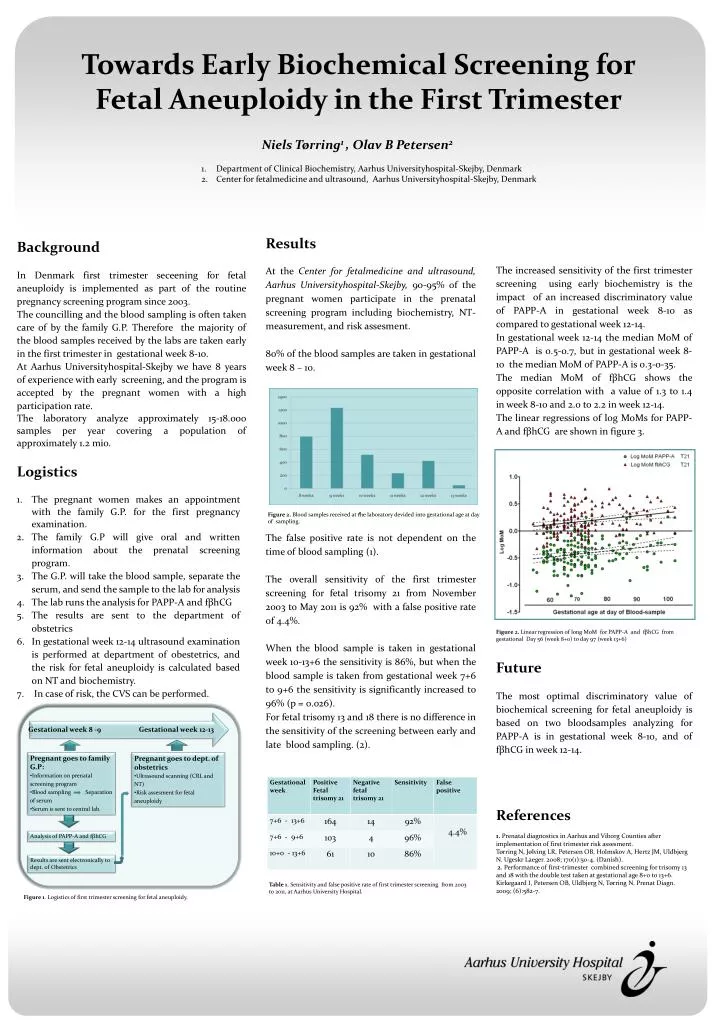
Towards Early Biochemical Screening for Fetal Aneuploidy in the First Trimester Results At the Center for fetalmedicine and ultrasound, Aarhus Universityhospital-Skejby, 90-95% of the pregnant women participate in the prenatal screening program including biochemistry, NT-measurement, and risk assesment. 80% of the blood samples are taken in gestational week 8 – 10. The false positive rate is not dependent on the time of blood sampling (1). The overall sensitivity of the first trimester screening for fetal trisomy 21 from November 2003 to May 2011 is 92% with a false positive rate of 4.4%. When the blood sample is taken in gestational week 10-13+6 the sensitivity is 86%, but when the blood sample is taken from gestational week 7+6 to 9+6 the sensitivity is significantly increased to 96% (p = 0.026). For fetal trisomy 13 and 18 there is no difference in the sensitivity of the screening between early and late blood sampling. (2). Background In Denmark first trimester seceening for fetal aneuploidy is implemented as part of the routine pregnancy screening program since 2003. The councilling and the blood sampling is often taken care of by the family G.P. Therefore the majority of the blood samples received by the labs are taken early in the first trimester in gestational week 8-10. At Aarhus Universityhospital-Skejby we have 8 years of experience with early screening, and the program is accepted by the pregnant women with a high participation rate. The laboratory analyze approximately 15-18.000 samples per year covering a population of approximately 1.2 mio. The increased sensitivity of the first trimester screening using early biochemistry is the impact of an increased discriminatory value of PAPP-A in gestational week 8-10 as compared to gestational week 12-14. In gestational week 12-14 the median MoM of PAPP-A is 0.5-0.7, but in gestational week 8-10 the median MoM of PAPP-A is 0.3-0-35. The median MoM of fβhCG shows the opposite correlation with a value of 1.3 to 1.4 in week 8-10 and 2.0 to 2.2 in week 12-14. The linear regressions of log MoMs for PAPP-A and fβhCG are shown in figure 3. Niels Tørring1 , Olav B Petersen2 1. Department of Clinical Biochemistry, Aarhus Universityhospital-Skejby, Denmark 2. Center for fetalmedicine and ultrasound, Aarhus Universityhospital-Skejby, Denmark • Logistics • The pregnantwomenmakes an appointmentwith the family G.P. for the firstpregnancyexamination. • The family G.P will give oral and written information about the prenatal screening program. • The G.P. willtake the blood sample, separate the serum, and send the sample to the lab for analysis • The lab runs the analysis for PAPP-A and fβhCG • The resultsare sent to the department of obstetrics • In gestationalweek 12-14 ultrasoundexamination is performed at department of obestetrics, and the risk for fetalaneuploidy is calculatedbasedon NT and biochemistry. • In case of risk, the CVS canbeperformed. 1 Figure 2. Blood samples received at the laboratory devided into gestational age at day of sampling. Figure 2. Linear regression of long MoM for PAPP-A and fβhCG from gestational Day 56 (week 8+0) to day 97 (week 13+6) Future The most optimal discriminatory value of biochemical screening for fetal aneuploidy is based on two bloodsamples analyzing for PAPP-A is in gestational week 8-10, and of fβhCG in week 12-14. References 1. Prenatal diagnostics in Aarhus and Viborg Counties after implementation of first trimester risk assesment. Tørring N, Jølving LR, Petersen OB, Holmskov A, Hertz JM, Uldbjerg N. Ugeskr Laeger. 2008; 170(1):50-4. (Danish). 2. Performance of first-trimester combined screening for trisomy 13 and 18 with the double test taken at gestational age 8+0 to 13+6. Kirkegaard I, Petersen OB, Uldbjerg N, Tørring N. Prenat Diagn. 2009; (6):582-7. Gestational week 8 -9 Gestational week 12-13 • Pregnantgoes to family G.P: • Information onprenatal screening program • Blood sampling Separation of serum • Serum is sent to central lab. • Pregnantgoes to dept. of obstetrics • Ultrasound scanning (CRL and NT) • Riskassesment for fetalaneuploidy Analysis of PAPP-A and fβhCG Resultsare sent electronically to dept. of Obstetrics Table 1. Sensitivity and false positive rate of first trimester screening from 2003 to 2011, at Aarhus University Hospital. Figure 1. Logistics of first trimester screening for fetal aneuploidy.