Download
1 / 29
320 likes | 370 Views
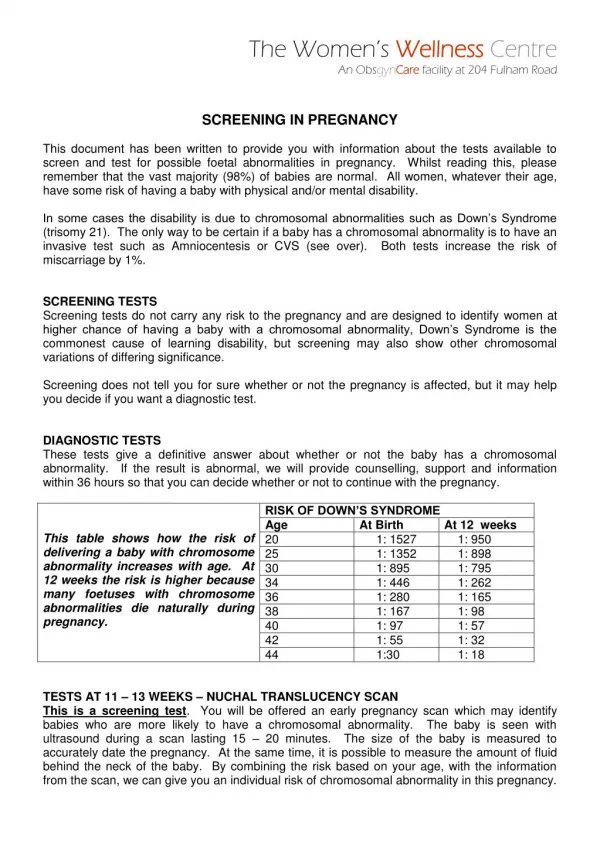
First Trimester screening in Multiple pregnancy. Firas Abdeljawad , MD Feto-Materanal Makassed Hospital Jerusalem. Multiple pregnancy. Screening for chromosomal abnormalities. Determination of chorionicity. Method of screening Maternal age Serum biochemistry

E N D
First Trimester screening in Multiple pregnancy FirasAbdeljawad , MD Feto-Materanal Makassed Hospital Jerusalem
Multiple pregnancy Screening for chromosomal abnormalities • Determination of chorionicity • Method of screening • Maternal age • Serum biochemistry • Nuchal translucency • Councelling • Method of invasive testing • Amniocentesis • Chorionic villous sampling • Discordance of abnormality • Selective fetocide • Expectant management
Multiple pregnancy Chorionicity and zygocity 9 twins 2/3 1/3 6 Dizygotic 3 Monozygotic All 2/3 1/3 7 Dichorionic 2 Monochorionic • All monochorionic twins are monozygotic • 6 of 7 dichorionic twins are dizygotic
Zygosity rather than chorionicity determines the of risk , and weather or not the fetuses may be concordant or discordant for chromosomal anomalies .
Detection rate for FPR 5% 100 90 80 70 60 50 40 30 20 15 20 25 30 35 40 45 50 10 Maternal age (yrs) 0 Screening for aneuploidies Maternal age Risk 1 in: 1 10 100 30% of fetuses with trisomy 21 in women >35 years 1,000 10,000
SingletonMC twins Age (yrs) DC twins Risk 1 in: Age >35 yrs 202530313233343536373839404142434445 1/10681/946 1/626 1/544 1/460 1/3801/3121/250 1/200 1/150 1/118 1/90 1/681/50 1/38 1/30 1/201/16 1/5341/483 1/313 1/272 1/230 1/1901/1561/125 1/100 1/75 1/59 1/45 1/341/25 1/19 1/15 1/101/8 1 Twins Age >32y 65% 35 % 30 10 28% 25 20 100 20% 15 1,000 10 5 10,000 15 20 25 30 35 40 45 50 0 Maternal age (yrs) Singleton Twins England & Wales 2007 Multiple pregnancy Screening for trisomy 21: Maternal age
In Twins , Effective screening for chromosomal abnormalities is provided by a combination of maternal age and fetal NT .
98% 100 % 90 80 70 60 50 40 30 20 10 0 Early screening for aneuploidies Age, ultrasound and serum ß-hCG & PAPP-A Detection rate for FPR 3%
n = 3945 n = 769 12 9 8 10 7 8 6 5 NT (mm) NT (mm) 6 4 4 3 2 2 1 0 0 35 45 55 65 75 85 35 45 55 65 75 85 Crown Rump Length (mm) Crown Rump Length (mm) Multiple pregnancy Screening for trisomy 21: Nuchal translucency DC: calculate risk for each MC: calculate average risk
Although 10 % of dichorionic twins are actually monozygotic and should have their risk calculated as such , this small percentage has not been found to affect overall screening accuracy in this population .
The performance of screening can be improved by the addition of maternal serum biochemistry , but appropriate adjustment are needed for chorionicity .
2.8 2.8 DC DC 2.4 2.4 2.0 2.0 MC 1.6 1.6 MC PAPP-A MoM free ß-hCG MoM 1.2 1.2 1.0 1.0 0.8 0.8 0.6 0.6 8 9 10 11 12 13 14 8 9 10 11 12 13 14 Gestation (wks) Gestation (wks) Multiple pregnancy Screening for trisomy 21: Serum free ß-hCG & PAPP-A Normal Tr 21 Include serum biochemistry, NICE 2011 Make appropriate adjustments 3.0 0.5 1.0 1.5 2.0 2.5 0.1 Free ß-hCG
Multiple pregnancy Diagnosis of aneuploidies Amnio vs CVS • Feasibility • Accuracy • Miscarriage • Embryo reduction
63% 12 wks 20 wks 57% <16 wks >16 wks • Miscarriage 14% • Delivery <33w 20% • Miscarriage 5% • Delivery <33w 6% 31% 24% 14% 14% 6% 6% 5% 0% Multiple pregnancy Timing of selective termination Loss 25 - 28 29 - 32 33 - 36 37- 42 Gestation at delivery (wks) Evans et al 1994
In monochorionic multiple pregnancies , an increased NT measurement had a high specifity and positive predictive value for adverse perinatal outcome .
Multiple pregnancy Chorionicity DC MC 2% 10% Miscarriage (11-23 weeks) 2% 4% Perinatal death (>23 weeks) 20% 30% Fetal growth restriction (>1) 5% 10% Preterm delivery (<32 weeks) 1% 4% Major defects 12 wks - anatomy, NT 16, 18 & 20 wks - TTTS, sFGR 22 wks - anatomy, growth, cervix 28, 32 & 36 wks - growth* yes - yes yes yes yes yes yes
The prediction of pregnancy complication is an important obstetric goal because it allows the perinatal team to make a decisions regarding antenatal management , including whether intervention is required , and timing of delivery .
Monochorionic twins Monochorionic twins Twin to Twin Transfusion Syndrome TTTS Selective Fetal Growth Restriction Twin reversed arterial perfusion sequence TRAP Frida Kahlo 1932 Twin Anemia-Polycythemia Sequence TAPS
Multiple pregnancy Monochorionic twins 1/6 1/6 Severe TTTS Selective FGR Frida Kahlo 1932
DONOR: UA - Absent / Reverse EDF RECIPIENT: DV Absent / Reverse a wave Endoscopic laser surgery for severe TTTS
Type I: normal Doppler Good prognosis Type II: AREDF Type III: iAREDF High rate IUFD neurological damage Multiple pregnancy Selective fetal growth restriction
60 Laser separation (n=118) Cord coagulation (n=18) % 50 40 30 20 10 0 PPROM Survival Both dead Multiple pregnancy Selective fetal growth restriction • Selective IUGR management options • Elective very preterm delivery • Laser separation of placental vessels • Selective fetocide of the small twin
MonochorioncDiamniotic twins , Early sign of severe selective IUGR • Refused selective fetocide at 12 weeks • IUFD of small fetus at 14 weeks • Now she is 18 weeks with …..
The most extreme manifestation of TTTS • Found in about 1% of MZ twin pregnancies Prematurity 75% Mortality 50% Moore et al, Am J Ob Gyn 1990: n=49 Multiple pregnancy Twin reversed arterial perfusion sequence Mortality: 25% Delivery <35 w: 30% Timing: 12 w vs 16 w
Multiple pregnancy Early anomaly scan Discordance for fetal abnormality Defects in DC = X1 singleton • Management options • Coservative • SelctiveFetocide • KCL DC • Laser MC Defects in MC = X4 singleton Discordance for defects:MC = DC
Singleton Births (%) Twin Triplet 30% 15% 1% 24 28 32 36 40 42 Gestation (wks) Multiple pregnancy Preterm delivery Singleton 100 • Prevention • No effect: • Bed rest • Cervical cerclage • Cervical pessary • Progesterone 75 Twins 1163 Triplets 43 Risk of delivery <34 wks (%) 50 25 0 0 10 20 30 40 50 60 Cervical length (mm)