Download
1 / 16
160 likes | 270 Views
Optimizing and simplifying the toolkit (drugs, dosing, and diagnostics) and delivery of ART. Dr Eric Goemaere Regional TB/HIV Advisor MSF South Africa. Bending the curves. Reducing clinical workload Bending the epidemic curve Distributing tasks

E N D
Optimizing and simplifying the toolkit (drugs, dosing, and diagnostics) and delivery of ART Dr Eric Goemaere Regional TB/HIV Advisor MSF South Africa
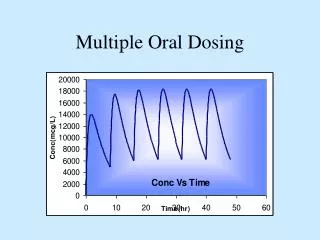
Bending the curves • Reducing clinical workload • Bending the epidemic curve • Distributing tasks • Increasing patient autonomy & adherence • Long term community based chronic care • Reducing pill burden and toxicities • ARV dosage optimization • New formulations • New ARVs
Patient-centered efficiency Increased coverage Lower Cd4 threshold Reduced clinical time /patient Patient friendly regimen: easy to use low toxicity, forgiving Doctors Patient self management PHC decentralised care, nurse based CHW supported
Bending the epidemic curve Moving from emergency to a chronic phase Transition needs to happen as soon as possible -> early aggressive approach ( emergency phase) Khayelitsha2001-2007
Distributing tasks Clinical screening Clinical screening Consultation Psycho social support Psycho social support Drug re-fill Drug re-fill
Pop. 500,000 (250,000 adults) ANC prevalence 30% =est. 60 -70,000 HIV+ Incidence =est. 4000 new infections/year What will Khayelitsha look like in 10 years ? 2009 2019
Thyolo, MalawiDecentralization to health posts Outreach from existing health centers if > 10 km Minimum package of HIV services ARV refills dispensed by lay health workers (HSAs) for stable patients on HAART Staffing: one community nurse and 2-3 HSAs
Tete, MozambiqueCommunity-HAART Groups • PLWHA driven • Support group w/ ART provision • Rep. Elecetd to collect ARV's • Maximum 6 patients • Between June 08 and Dec 09 • 199 CHG formed 1253 patients • 95.4 % RIC • 1.7 % died • 0.2 % LTFU • 1.9 % TFO • 0.8 % returned to HC
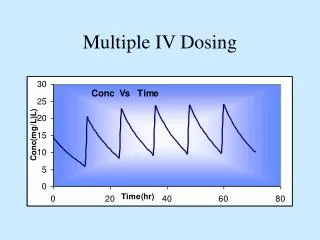
Dose optimization • Objectives: • Reduce patient toxicity • Reduce pill burden • Reduce costs • d4T: from 40 mg to 30 mg BID dose for all patients • AZT was initially marketed as 250mg bid in Europe until late 1990s. Dose still available for sale in Europe • For several HIV drugs, Phase 2 data showed no difference in efficacy between doses, but higher doses were selected for Phase 3 and registration (EFV, LPV/r, RAL, 3TC) • In drug development, dosage selection is made early and not reassessed later
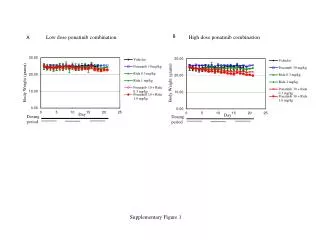
Reducing D4T dosage Impact on regimen safety Source: Charlotte Schultz , GFJooste ID referral unit, cape Town
Potential Dose Optimization Investigations _________________________________________________________ Drug Current dose Target Optimised dose _________________________________________________________ ZDV 300mg BID 200 mg BID 3TC 300 mg OD 150 mg OD ** EFV 600 mg OD 400 mg OD ** LPV/r 400/100 mg BID 200/100 or 200/150 BID ** ATV/r 300/100 mg OD 300/50 or 200/50 mg OD DRV/r 600/100 BID 400/50 mg OD (PI naives) RTV 100mg (booster) 50mg (booster) RAL 400mg BID 100-200 mg BID _________________________________________________________ ** Encore trials : funded and support from Bill and Melinda Gates Foundation, University of New South Wales and Clinton Health Action Initiative Source: Andrew Hill
Long term therapeutic strategy • Specific treatment paradigm for high prevalence LRC contexts ? • Future perspectives • Moving away from a sequential paradigm to Induction/maintenance paradigm ? • Drug required profile • Potent regimen for induction ( Raltegravir/Darunavir/r) • Systematic switch to maintenance with no monitoring • Long half life, forgiving regimen( PI based ) for maintenance • Safe, minimal side effects , • NRTI sparing
New drugs,new formulations? • Promising drugs • Rilpivirine (Tibotec) – NNRTI, (Phase III) • low dose 25mg, long half life 38 hours, • Elvucitabine (Achillion) – NRTI, (Phase II) • low dose 10mg, long half life 49hrs, safety efficacy data? • CMX 157 (Chimerix) – (Phase I), • prodrug of TDF,more potent than TDF++, low dose, safety efficacy data? • S/GSK 1349572 (ViiV) (Phase IIb) • – Integrase Inhibitor, low dose 50mg, no booster required, long half life 30 hours, safety efficacy data?