Download
1 / 34
390 likes | 759 Views
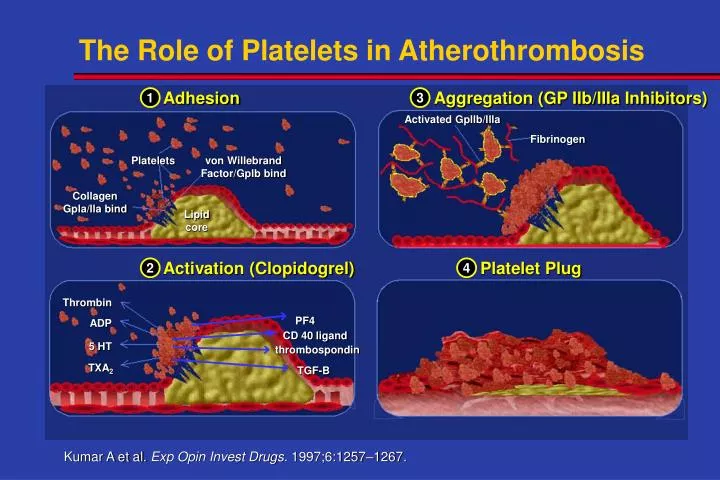
The Role of Platelets in Atherothrombosis. Adhesion. Aggregation (GP IIb/IIIa Inhibitors). 1. 3. Activated Gpllb/llla. Fibrinogen. von Willebrand Factor/Gplb bind. Platelets. Collagen Gpla/lla bind. Lipid core. Platelet Plug. Activation (Clopidogrel). 2. 4. Thrombin. PF4. ADP.

E N D
The Role of Platelets in Atherothrombosis Adhesion Aggregation (GP IIb/IIIa Inhibitors) 1 3 Activated Gpllb/llla Fibrinogen von Willebrand Factor/Gplb bind Platelets Collagen Gpla/lla bind Lipid core Platelet Plug Activation (Clopidogrel) 2 4 Thrombin PF4 ADP CD 40 ligand 5 HT thrombospondin TXA2 TGF-B Kumar A et al. Exp Opin Invest Drugs. 1997;6:1257–1267.
IV Gp IIb/IIIa Inhibitors in ACS: Death or MI at 30 Days (N=31,402) 95% CI Study Placebo IV Gp IIb/IIIa Odds Ratio PRISM 7.1% 5.8%† 0.80 0.60-1.06 PRISM-PLUS 12.0% (*) 8.7% 0.70 0.50-0.98(† ) 13.6%† 1.17 0.80-1.70 PARAGON-A 11.7% (l) 10.3% 0.87 0.58-1.29(h) 12.3% 1.06 0.72-1.55 PURSUIT 15.7% (l) 13.4% 0.83 0.70-0.99(h) 14.2% 0.89 0.79-1.00 PARAGON-B 11.4% 10.6% 0.92 0.77-1.09 GUSTO-IV 8.0% (24h) 8.2% 1.02 0.83-1.24(48h) 9.1% 1.15 0.94-1.39 Overall 11.8% 10.8%* 0.91 0.85-0.99 0.0 1.0 2.0 P=.015 Gp IIb/IIIa Better Placebo Better † without heparin, * with/ without heparin (l) = low dose, (h)= high-dose Boersma, E. et al. Lancet. 2002;359:189-198. Odds Ratio (95% CI) srm
IV GP IIb/IIIa Inhibitors in ACS: Death or MI (at 30 d): Subgroup Results Boersma, E. et al. Lancet. 2002;359
IV GP IIb/IIIa Antagonists in ACSDeath or MI (at 30d) by PCI/CABG < 5 days P=0.001 P=NS Interaction p < 0.02 N=25,555 N=5847 Boersma et al. Lancet 2002; 359: 189b
PRISM 1.2% 1.7% † 1.36 0.76-2.43 PRISM-PLUS 2.0% 3.0% 1.50 0.78-2.86 PARAGON-A 0.7% 1.3% 2.02 0.58-7.03 PURSUIT 0.9% 1.1% 1.33 0.75-2.34 PARAGON-B 1.0% 1.7% 1.79 1.10-2.93 GUSTO-IV 2.8% 4.7% 1.72 1.28-2.32 Overall 1.4% 2.4%* 1.62 1.36-1.94 IV Gp IIb/IIIa Inhibitors in ACS: Major Bleeding at 30 Days Odds Ratio Study Placebo IV Gp IIb/IIIa 95% CI † without heparin, * with/ without heparin major bleeding for all low dose treatment Boersma, E. et al. Lancet. 2002;359:189-198. srm
Death During Follow-up Period N Odds Ratio & 95% CI Placebo Fiban Trial 7,232 EXCITE 0.3% 0.7% 2.14 Xemilofiban 10,302 OPUS 1.4% 2.0% 1.40 Orbofiban 9,169 SYMPHONY 1.8% 2.0% 1.14 Sibrafiban 6,637 2nd SYMPHONY 1.3% 2.1% 1.55 Sibrafiban Pooled 1.3% 1.7% 33,340 1.37 p = 0.002 0.5 1 1.5 2 0 Fiban Better Fiban Worse p = 0.588 Breslow-Day heterogeneity Chew DP, Bhatt DL, Sapp S, and Topol EJ. Circulation.2001;103:201-206. Chew DP, Bhatt DL, Sapp S, and Topol EJ. Circulation. 2001;103:201-206.
Synergistic Antithrombotic Effect of Clopidogrel Plus Aspirin in Humans Ex vivo study of collagen-induced thrombus formation in 18 healthy volunteers at day 10 6 Baseline ASA 325mg 5 C 75mg+ ASA 325mg 4 C 300mg+ ASA 325mg 3 Platelet deposition (x10-7/cm2) 2 ** ** 1 0 Baseline ASA C75+ASA C300+ASA ** p <0.01 vs ASA. Cadroy et al. Circulation. 2000;101:2823-2828.
Rapid Platelet Inhibition ofClopidogrel* 375 mg Loading Dose 100 91 85 80 80 79 80 68 55 60 Percent (%) Inhibition (5 mcM ADP) 40 19 20 0 0 Day 1, Day 1, Day 1, Day 1, Day 1, Day 2 Day 3 Day 5 Day 10 0hr 0.5hr 1.0hr 2.0hr 5.0hr * Clopidogrel 75mg/d given on days 2-10. Bachmann F et al. Eur Heart J. 1996;17(suppl):263. Abstract.
Efficacy of Dual Antiplatelet Therapy vs ASA alone in Reducing Coronary Events after Stenting Death or MI Study Odds Ratio 95% CI HALL (1996) 0.17 0.25 0.23 0.01-0.72 0.10-0.63 0.11-0.49 *STARS (1998) Total P=0.0001 10.0 0.1 1.0 ASA alone Better ASA + Ticlopidine Better Test for heterogeneity P=0.66 *STARS was a 3 arm trial. Data for aspirin + ticlopidine vs aspirin alone were used for this analysis. Mehta et al. for The CURE Study Investigators. Eur. Heart J. 21 ;24, 2000.
Efficacy of Dual Antiplatelet Therapy vs Warfarin and ASA in Reducing Coronary Events after Stenting Death or MI Study Odds Ratio 95% CI ISAR (1996) 0.31 0.32 0.61 0.66 0.51 0.11-0.91 0.11-0.91 0.26-1.43 0.33-1.30 0.33-0.78 *STARS (1998) MATTIS (1998) FANTASTIC (1998) Total P=0.002 10.0 0.1 1.0 ASA + Oral Anticoagulation Better ASA + Ticlopidine Better Test for heterogeneity P=0.51 *STARS was a 3 arm trial. Data for aspirin + ticlopidine vs aspirin Mehta et al. for The CURE Study Investigators. Eur. Heart J. 21 ;24, 2000.
MI/Stroke/CV Death/Severe Ischemia Within 24 hrs of Randomization Cumulative Hazard Rates 0.025 Placebo + ASA 0.020 34% Relative RiskReduction 0.015 Clopidogrel + ASA 0.010 0.005 RR= 0.66 =0.003 p 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 Hours After Randomization Mehta SR et al. AHA, 2002
Interventions Associated with Refractory Ischemia in Hospital
Benefit of Clopidogrel stratified by TIMI Risk Score ARR 1.6% 1.6% 4.8% P=0.003 P=0.02 P=0.03 N=3276 N=7297 N=1989 Budaj et .al Circulation, In Press
Prevention of large MI, thrombolytic use and new onset CHF after randomizaton Placebo + ASA*N = 6303 Clopidogrel + ASA*N = 6259 Relative Risk Reduction Outcome P value • Q-wave MI 3.1% 1.9% 40% <0.001 • Thrombolytics 2.0% 1.1% 43% < 0.001 • Heart Failure‡ 4.4% 3.7% 18% 0.03 * In addition to other standard therapies ‡ Radiologically confirmed
CV Death/MI Among Patients Undergoing Early PCI (< 72 Hrs) RRR 38% RRR 29% N=544 N=2114 Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
PCI-CURE CV Death or MI at Various Intervals RRR 31% 32% 34% 21% * *P=0.002 Mehta, SR. et al for the CURE Trial Investigators. Lancet. August 2001;21:2033-41.
Benefit/Risk Ratio Yusuf, Mehta. N Eng J Med 2002; correspondence
CURE Study Definition of Bleeding • Bleeding was defined as “Major” or “Minor” • Major bleeding was defined as follows: • requiring at least 2 units of blood, substantially disabling, or intraocular bleeding leading to vision loss • Major Bleeding was sub-categorized as life-threatening if it was: fatal, symptomatic intracranial hemorrhage, leading to a drop in hemoglobin of at least 5 g/dL, significant hypotention requiring IV inotropes, requiring surgical intervention, or requiring transfusion of 4 or more units of blood • Minor • any other bleeds that led to interruption of study medication The CURE Trial Investigators. N Engl J Med. 2001;345:494-502.
TIMI Major Bleeding / GUSTO Severe-Life-Threatening Bleeding Criteria
Bleeding by GP IIb/IIIa Use % Events
Number and Proportion of Patients Undergoing Cardiac Procedures in ACS Trials SMR
Relative Benefits of Different Interventions in ACS By Time (Death/MI) Long term benefits from lipid lowering and ACE-inhibitor therapy
Risk-Benefit Analysis of Clopidogrel versus IV GP IIb/IIIa in ACS Active Placebo ARR P value * † *Yusuf S, Mehta SR. N Engl J Med 2002 (correspondence). †Boersma, E. et al. Lancet. 2002;359:189-198
Benefit-Risk Comparison of Antithrombotic Therapies vs Placebo in UA/NSTEMI Treatment Major Duration N Death or MI Bleeding * In addition to aspirin † reported death or MI at 150 days 1. Antithrombotic Trialists’ Collaboration. BMJ 2002;324:71-86 2. The CURE Trial Investigators. NEJM 2001;345:494-502. 3. Frisc Investigators. Lancet 1996;347:561-568. 3..4. Boersma E, et al. Lancet 2002;359:189-198. Mehta SR. JACC 2002, In Press
CURE: 12562 1.5% 2.0% +0.5% IV GP IIb/ IIIa Trials: PRISM-PLUS 1915 0.8% 1.4% +0.6% PURSUIT 9375 9.1% 10.6% +1.5% CAPTURE 1265 1.9% 3.8% +1.9% Major Bleeding in IV GP IIb/IIIa Antagonists ACS Trials vs CURE: Within 30 Days Trial N Placebo* Active* Diff * In addition to other standard therapies including aspirin and heparin. The CURE Trial Investigators. N Engl J Med. 2001;345:494-502. The PRISM-PLUS Study Investigators. N Engl J Med. 1998;338:1488-97.The PURSUIT Trial Investigators. N Engl J Med. 1998;339:436-443.The CAPTURE Investigators. Lancet. 1997;349:1429-1435. Mehta S. J Am Coll Cardiol. In Press
Role Of Antiplatelet Therapies In ACS: • Both ASA (RR of 40%) and clopidogrel (RR of add’l 20%) should be initiated early and continued long term, and are effective in addition to standard therapies (heparin, GP IIb/IIIa inhibitors and interventions) • GP IIb/IIIa inhibitors (RR of 9% at 30 days) is best reserved for patients undergoing PCI • All antiplatelet agents increase the risk of CABG related bleeds. Therefore an individualized approach (to the timing of CABG, continuation or discontinuation of the antiplatelet agents, the need for platelet transfusion) depending on the urgency of CABG and severity of CAD is needed • Pre-treatment of patients with ASA and clopidogrel and periprocedural (PCI) use of IV GP IIb/IIIa inhibitors substantially reduces the risk of Death/MI
State of the Art Management ofnon-ST ACS • Acute • ASA + Clopidogrel • LMWH/UFH • IV GP IIb/IIIa inhibitor during PCI for those undergoing an invasive strategy (moderate to high risk patients) • Long Term • ASA + Clopidogrel for at least one year • Planned program of secondary risk factor modification including smoking cessation, lipid lowering therapy, ACE inhibitor, BP and diabeticcontrol, weight reduction
Implications of CURE and PCI CURE The results from both CURE and PCI CURE suggest that a broad range of patients with non-ST elevation ACS who present with ischemic ECG changes or positive enzymes will benefit with treatment with ASA and clopidogrel, in addition to other standard therapies, regardless of their baseline risk or management strategy