Download
1 / 40
400 likes | 412 Views
Hypokalemia is a condition characterized by low potassium levels in the body. This can have profound effects on cardiovascular and neuromuscular systems. Learn about the causes, effects, and treatment options for hypokalemia.

E N D
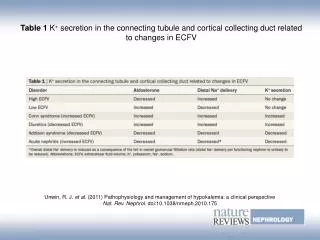
INTRODUCTION • Potassium is one of the body's major ions. • Nearly 98% of the body’s potassium is intracellular. • The ratio of intracellular to extracellular potassium is important in determining the cellular membrane potential. • Small changes in the extracellular potassium level can have profound effects on the function of the cardiovascular and neuromuscular systems. • The kidney determines potassium homeostasis, and excess potassium is excreted in the urine.
INTRODUCTION • potassium is necessary for the maintenance of normal charge difference between intracellular and extracellular environments. • potassium homeostasis is tightly regulated by specific ion-exchange pumps (primarily by a cellular, membrane-bound, sodium-potassium ATP-ase). • Derangements of potassium regulation often lead to neuromuscular, gastrointestinal, and cardiac conduction abnormalities.
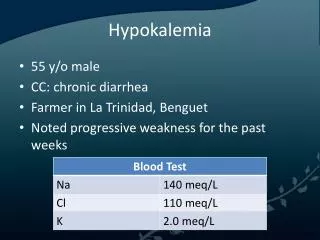
Definition • Hypokalemia is defined as a potassium level less than 3.5 mEq/L. • Moderate hypokalemia is a serum level of 2.5-3 mEq/L. • Severe hypokalemia is defined as a level less than 2.5 mEq/L. The reference range for serum potassium level is 3.5-5 mEq/L
PATHOPHYSIOLOGY chronic inadequate intake, long-term diuretic or laxative use, chronic diarrhea, hypomagnesemia & hyperhidrosis Total body deficit of potassium diabetic ketoacidosis, severe GI losses : vomiting / diarrhea, dialysis, and diuretic therapy Acute potassium depletion potassium shifts from the EC to IC space Alkalosis & hypothermia insulin, catecholamines Distal RTA & Bartter syndrome, Periodic hypokalemic paralysis, Hyperaldosteronism & hyperthyroid. Other causes
Abnormalities of serum potassium are associated with well described clinical features: Gennari FJ. Hypokalemia. N Engl J Med 1998; 339: 451-458
Effects of hypokalemia • Atrial/ventricular Arrhythmiasare more common in patients with underlying heart disease (especially CAD) and in patients taking digoxin. • life-threatening Cardiac Arrhythmias can occur when the serum potassium is very low (< 2 meq/L), or when the serum potassium is relatively low (2 - 3 meq/L) in patients with underlying heart disease, or when the patient is digoxin-toxic.
Effects of hypokalemia • severe (or rapidly occurring) hypokalemia can cause muscle weakness and paralysis the paralysis mainly affects the proximal lower extremities => progressing to affect the upper extremities; dysphagia and dysarthria are uncommon and cranial nerve palsies are exceedingly rare) • Rhabdomyolysis can occur in severely potassium-depleted patients - especially following vigorous exercise - and muscle necrosis can rarely occur
Effects of hypokalemia • hypokalemia produces a carbohydrate-intolerance(? due to impaired insulin release and ? impaired insulin resistance) => worsening hyperglycemia in diabetics. • hypokalemia also produces a metabolic alkalosis (by ? stimulation of bicarb absorption by the proximal tubule and ? renal ammoniagenesis) • hypokalemia can contribute to the development, or worsen the symptoms, of hepatic encephalopthy(? due to renal ammoniagenesis)
Investigations • Although ECG changes may be helpful if present, their absence should not be taken as reassurance of normal cardiac conduction. The ECG in hypokalemia may appear normal or may have only subtle findings immediately prior to clinically significant dysrhythmias. • During therapy, monitor for changes associated with over-correction and hyperkalemia including prolonged QRS, peaked T waves, bradyarrhythmia, sinus node dysfunction, and asystole.
The ECG findings in hypokalemia: Ventricular dysrhythmia, Prolongation of QT interval, ST segment depression, T wave flattening& U waves.
Investigations • Drug screen (serum or urine): • Amphetamines and other sympathomimetic stimulants can cause hypokalemia. • Other drugs include • verapamil overdose. • Theophylline. • amphotericin B. • Aminoglycosides. • cisplatin. • Hormonal assay: • Serum ACTH, • Cortisol, • Renin activity, • Aldosterone
left adrenal adenoma Conn syndrome
2. Replenishing potassium stores There is no direct correlation between the serum potassium and the total body potassium deficit, but a rough estimate is to assume a total body deficit of ~ 200 - 400 meq of potassium for every 1 meq/L the serum potassium is below 4 meq/L consider the possibility of associated magnesium deficiency
Replenishing potassium stores cardiac monitoring is necessary in patients with • profound hypokalemia (< 2.5 meq/L), or • if cardiac arrhythmias are present, or • if IV potassium is going to be rapidly administered. IV potassium should normally be diluted in saline solution so that the maximum concentration is 40 meq/L (peripheral lines) or 60 meq/L (central lines) and IV potassium.
Medical Decision-Making and Treatment • Transient, asymptomatic, or mild hypokalemia may resolve spontaneously or may be treated with enteral potassium supplements. • Potassium replacement therapy is immediately indicated for: • Severe hypokalemia (< 2.5 meq/L), or • If the hypokalemia is causing muscle paralysis, or • Malignant cardiac arrhythmias .
Medical Decision-Making and Treatment • Outpatient therapy and follow-up in 48 - 72 hours may be acceptable for mild hypokalemia patients with no underlying heart disease.
Medical Decision-Making and Treatment The patient should be transferred to ICU for severe or symptomatic hypokalemia for: • IV potassium supplementation. • Continuous cardiac monitoring.
Magnesium Replacement Therapy • Magnesium replacement therapy is often necessary in malnourished alcoholics with hypokalemia. • Hypomagnesemia should be suspected if the serum potassium does not increase within ~ 96 hours of the commencement of potassium supplementation therapy. • Magnesium can be given orally (3g x 4 doses).
what is the next step? The cause of hypokalemia
Certain simple combinations of clinical features and abnormal laboratory values could suggest a particular diagnosis
Q.1. Hypertension + High Serum Renin + High Serum Aldosterone. • Renin secreting tumor or • Bilateral renal artery stenosis or • Malignant hypertension
Q.2. Hypertension + Low Serum Renin + High Serum Aldosterone. Primary Hyperaldosteronism
Q.3.Hypertension + Low Serum Renin + Low Serum Aldosterone. • Liddle syndrome or • congenital adrenal hyperplasia or • chronic ingestion of licorice-compounds containing glycyrrhizin or • ingestion of other exogenous mineralocorticoids
Q.4.Hypertension + Normal/high Serum Renin + Normal Serum Aldosterone Cushing’s Syndrome
Q.5. Hypotension/normotension + High Serum Renin + High Serum Aldosterone. “Secondary Hyperaldosteronism”
Q.6. Normotension + metabolic acidosis + hyperchloremia + urine ph > 6. Distal RTA
Bartter's syndrome Q.7. Normotension/hypotension Increased serum renin Metabolic aklalosis Hypomagnesemia Hypercalciuria Increased urinary chloride (> 100 meq/l)
Q.8. Normotension/hypotension + metabolic alkalosis + low urinary chloride • Surreptitious vomiting or • Prolonged naso-gastric suction and excessive gastric fluidloss
Surgical Care • Surgical intervention is required only after determining that the etiology requires it. • Etiologies that may require surgery include the following: • Renal artery stenosis. • Adrenal adenoma. • Intestinal obstruction producing massive vomiting. • Villous adenoma.
Consultations The following consultations may be appropriate, depending on the clinical findings: • Nephrologist for evaluation of unexplained urinary potassium losses suggested to be secondary to a tubular disorder. • Endocrinologist if Cushing syndrome, primary hyperaldosteronism, glucocorticoid-remediable hypertension, or congenital adrenal hyperplasia is suggested. • Psychiatrist for alcoholism or eating disorders • Surgeon.
Diet: ‟low-sodium and high-potassium” The low-sodium diet limits the amount of sodium reabsorbed at the cortical collecting tubule, thus limiting the amount of potassium secreted.
Further Inpatient Care • Matching potassium intake to losses. • Monitoring for Hypokalemia or Hyperkalemia Due to Therapy By: • periodic testing of serum potassium levels • EKG. • Alleviation of aggravating conditions.
Further Outpatient Care • Patients should receive follow-up medical care for home management if the condition is expected to persist beyond inpatient care. • Additional medical follow-up must be obtained for associated medical conditions.
Patient Education • Patients should be educated in terms of predisposing conditions. • The importance and risks involved with potassium supplementation and • The warning signs of hypokalemia or over-treatment must be emphasized in discharge teaching. • Knowledge of cardiopulmonary resuscitation and education on timely access to emergency medical services may prevent morbidity or mortality. • Ongoing communication is essential in reducing the risks and therapy, especially in patients with chronic conditions associated with hypokalemia.
Medical/Legal Pitfalls • Failure to adequately communicate the risks of treatment • Failure to appropriately monitor patients receiving potassium supplementation for complications, • Failure to follow serum potassium and other electrolyte concentrations during or after therapy • Treating a patient based on a falsely low serum potassium value due to sampling or lab error