Download

1 / 50
500 likes | 517 Views
Learn about patient preparation, contraindications, contrast dosing, equipment instrumentation, imaging protocol, and reconstruction techniques for accurate results in coronary CT angiography.

E N D
Introduction • 64-slice coronary CT angiography is highly accurate for the exclusion of significant coronary artery stenosis (>50% luminal narrowing) • with negative predictive values of 97%–100%, in comparison with invasive selective coronary angiography.
INTRODUCTION • patient preparation • image acquisition • evaluation techniques
Patient Preparation, Contraindications, Contrast Dosing Patient Preparation
Patient Preparation • Image quality improved at low heart rates (<65 beats per minute). • Following steps can affect the heart rate: • The inspirational breath hold (-6beats/min) • oral ß-blocker (50—100mg oral or 5–20 mg I.V. Metoprolol) • Short-acting nitroglycerin (selective coronary angiography ) • The Lab GFR,BUN & Creatinin reports should be brought • The Diabetic Patients should stop Metformin administration 48hours prior and post the examination (if GFR and Creatinin is normal)
Patient Preparation • If GFR<30, the examination should be stopped. • Lidocaine / Xylocaine can be used for the correction of AF arrhythmia (PVC) • For rapid AF rhythm, Digocsine can be useful (under the supervision of a cardiologist) • The patient should be NPO for at least 6-8 hours. • Supine position • Sedation for children
Patient Preparation • For the administration of CM, two Types of Angiocaths are used: • Green • Pink
Patient Preparation • For CABG patients, in order to evaluate the LIMA origin, the IV line should be taken from the right hand. • How much the IV line diameters be narrower, the probability of extravasation increases. • The Examination procedure and the effects of breath holding should be explained to the patients. • The breath holding should be exercised with the patients for at least 2 times.
Patient Preparation • The patient lays supine on the table and the IV line adheres to the injector correctly. • Just before the examination starts, the NG spray/perlshould be administrated sublingually.
Contrast Dosing • Contrast volume is determined empirically based on patient weight • Nonionic isosmolar contrast medium is often used: 350-370 mg IC. • Dose: 1.5-2 mL/kg • Injection Rate: minimum 5-7 ml/s. • The injection must be done by dual supply injectors. For wash out of the right heart, the post-CM normal saline injection is recommended, in order to reduce the right heart artifacts on RCA.
Instrumentation, Imaging protocol Image Acquisition
Instrumentation • 64 up to 384 MDCT Instrumentation can be used. • The imaging time is reduced in higher detector array lengths. • The minimal equipment requirement for state-of-the-heart coronary CTA is a 64-slice scanner.
Instrumentation 10 mm detector Pitch ~0.25 3 cm in 5 sec 20 mm detector Pitch ~0.25 6.2 cm in 5 sec 40 mm detector Pitch ~0.25 12.5 cm in 5 sec
Imaging Protocol • Topogram • Calcium Scoring (Prospective) • Timing for the scan starting • Test Bolus • Bolus Tracking • CTA (Sequential/Spiral/FLASH) • MIP, VRT, MPR Reconstruction
Calcium Scoring (Prospective) • The calcium scale (mg/cm^3) is a linear scale with 4 calcium score categories: • 0 none • 1–99 mild • 100–400 moderate >400 severe • Calcium score correlates directly with risk of events and likelihood of obstructive CAD
Test Bolus • Primary injection :12-20 ml dye, 5-7 ml/s. • Loading the data into the DynEv. Software. • Drawing a ROI at the ascending Aorta level. • Addiction of Time-To-Peak (TTP) with 13 ms.
Bolus Tracking • Adjusting the Pre-monitoring at the level of Ascending Aorta. • Selecting the HU threshold to the 160 HU with the scanning interval of 1 ms, for the duration of 50 scans.
Retrospective, Prospective EKG Gating
R-R Interval 0% R-R Interval 100% 1000ms The percentage of reconstructions is based on the EKG signal temporal situation
ECG Gating • -Prospective ECG triggering • - Retrospective ECG gating • - Prospective ECG triggered spiral mode or f lash spiral cardiac mode • To obtain cardiac images with minimal motionArtifacts , data acquisition and image reconstructionically performed during the diastolic phaseOf the cardiac cycle Flashmode estimation phase 60 table speed delay 60 60 Scan acceleration time ti time trigger of table acceleration by CPI
Retrospective ECG triggering: • X-ray data are acquired throughout the entire Cardiac cycle. • Only data acquired during the cardiac phase with the least motionare used for image reconstruction.
Sequential ECG triggering: • X-ray data are acquired only throughout multiple Diastolic Cardiac cycles. • In this type of gating, the patient dose becomes lower than Retrospective type.
FLASH ECG triggering: • X-ray data are acquired only throughout oneDiastolic Cardiac cycle. • In this type of gating, the patient dose becomes lower than sequential type.
Techniques to Reduce Radiation HigherKV Imagecontrast noise dose LowerKV dose SNR (Contrast) SNR (Contrast) dose noise mAs
Low Dose Radiation of Coronary CTA mAs MAX 20% mM 20% mM
Min Dose Radiation of Coronary CTA mAs MAX 4% mM 4% mM
Care Dose Radiation of Coronary CTA: • It detects the radiation Dose on the topogram scans. • Based on topograms and the body thickness, the scanner changes the mAs.
Care KV of pediatric CTA: • It can be switched on or off. • When it is on, it reduces the kv to the lowest possible KV, in order to decrease the patient receiving dose. • It is usually used in children and pediatric patients.
Data Reconstruction • After the data acquisition, the image reconstructions are made based on EKGgating, with different percentages. • Form the reconstructed images, 3D and 2D (MPR, MIP, Curve, VRT) are acquired.
Data Reconstruction • In image reconstructions, BEST DIASTOLE and BEST SYSTOLIC phases should be made. • If any lesion in any percentages is noticed, for the confirmation, it should be evaluated at least in 2 other percentages.
Data Reconstruction • If any section from any artery will not be sharp in any percentage, for acquiring the best quality and the best percentage for that artery, the Preview technique is utilized.
MIP & VRT Reconstruction • In order to evaluate the lesions, both MIP and MPR techniques are used. Specially the sections with a high calcium content, MPR can help more. • If the presentation of any artery’s distance is required in a single line shape – with no curvature – the CURVE technique is used. For the presentation of every coronary arteries, the curve technique should be used by the Coronal, Sagittal, and Axial planes.
MIP & VRT Reconstruction • VRT technique is mostly utilized for the cardiac Anatomy, arterial malformations, arterial course, and a nice presentation of the heart. • For the stenosis determinacy evaluations, the VRT images are not in use.
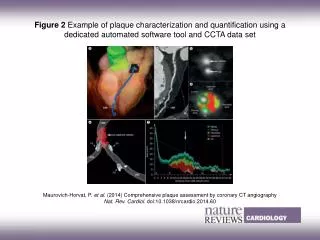
Artifact • Motion Artifacts: Occur at high rates and most often in the midsegment of the right coronary artery • Misalignment and Slab Artifacts: High heart rates, Heart rate variability, and the presence of irregular or ectopic heart beats (e.g. PVC, AF, Arrhythmia) • Blooming Artifacts:High-attenuation structures, such as calcified plaques or stents, appear enlarged (or bloomed) because of partial volume averaging effects and obscure the adjacent coronary lumen, the main cause of false-positive results in coronary CTA because of overestimation of the degree of stenosis
Motion Artifact at High HR (76 Rate/min). • Curved MPR image of the Artery with Heart Rate Motion Artifact. • Stair-Step Artifact related to Arrhythmia.