Download
1 / 32
330 likes | 463 Views
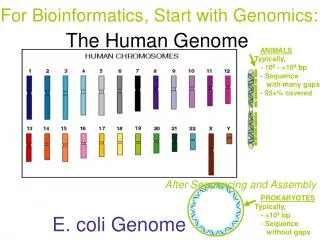
Verotoxigenic E. coli in West Limerick. Tessa Greally Acting Director of Public Health, HSE MWA on behalf of the Multidisciplinary Outbreak Control Team. June 2006. Verotoxigenic E. coli ( VTEC). Commensal in cattle Infection in humans first recognised in 1982

E N D
Verotoxigenic E. coli in West Limerick Tessa Greally Acting Director of Public Health, HSE MWA on behalf of the Multidisciplinary Outbreak Control Team June 2006
Verotoxigenic E. coli (VTEC) • Commensal in cattle • Infection in humans first recognised in 1982 • Commonest is E. coli O157 also O26, O111 • MWA 8-10 cases per year • Ireland 86 cases in 2003, increasing numbers in Ireland during 2005 (HPSC) • Outbreaks • Walkerton, Canada 2000, 2300 ill, 27 HUS, 7 deaths • Scotland 1996, 17 HUS deaths • Wales 2005, 1 death
Epidemiology • Young and old most affected • Transmission (V. low infective dose) • Direct contact with animals • Animal faeces in environment • Person to person spread • Contamination of water, or food • Incubation 1-8 days (usually 2-4 days) • Need for microbiological clearance in “at-risk” groups before return to work/school
VTEC Outbreak,West Limerick, 2005 • Mid Western Area, Ireland • (pop 340,000) • 8-10 cases of VTEC per year.
Outbreak Area/ West Limerick • Small rural area –cattle • pop. 1500 • Commuters • Private Group water scheme (600 people) • Boil water notice • Recent Slurrying • Heavy Rain
Dept of Public Health, MWHA October 2005 • 1 Acting DPH ( since 01/09/2005) • DPH transferred to national A/ND post without replacement • I Acting SPHM • 1 SpR • 1 Senior Medical Officer( SMO)( on MPH leave) • 1 Surveillance Scientist • 1 Temporary SMO from Australia( covering MPH leave for SMO) • 3 Community AMOs not transferred Split site
Index case- Tuesday Oct 25, 2005 Limerick PHU advised of a 2 year old child from West Limerick with HUS in Temple St Hosp • Recent history of diarrhoeal illness with negative stool result at local hospital • Risk factors • Attended local un-notified creche • Group Water Scheme serving creche under `”unfit” notice • Creche on a farm Contact screening of faeces undertaken according national guidelines
National screening guidelines Microbiological screening of faeces of : • All symptomatic close contacts • All household contacts • At risk groups-food handlers • Health care • Children < 5 years at nurseries, playgroups etc • Older children and adults unable implement good standards hygiene
Cluster 1 • Screening of creche, playgroup, junior infants class at school (<5), families of cases. • Index confirmed E.coli O157 VT2+ve (VTEC) • 8 contacts E.coli O157 VT2+ve, 4 symptomatic • 1 childminder, • 4 child-minding children<4 yrs, • 3 family contacts of index (incl Sibling-a schoolchild aged 4 years)
Cluster 2 • Child (10 yrs) from West Limerick attended A/E in Dublin • with bloody diarrhoea but not admitted • Public Health informed on November 2, 2005 in effort to trace case • Attended local school • Confirmed E.coli O157 VT2+ve • Only link mother had briefly looked after index case in hospital, asymptomatic • Mother negative • Also lived on another GWS and had visited farm in Cork recently with 2 wells • Father subsequently developed bloody diarrhoea E.coli O157 VT2+ve.
Cluster 3 • 2 yo from same area admitted bloody diarrhoea • Developed HUS -Peritoneal Dialysis. • Public Health notified November 15, 2005 • Attended another un-notified creche • 6 contacts E.coli O157 VT2+ve (1 symptomatic) • 3 child-minding children <4 years ( living on GWS1) • 3 family contact s (father of child with HUS , 2 siblings of child minding case) • No contact with other 2 clusters
Epidemiological investigation • Multi-disciplinary OCT convened 02/11/2005 • Case finding • Local GPs, paediatricians, emergency department alerted • Screening of 167 contacts including: • 2 Creches • 1 Playgroup contacts • Families of those affected • School contacts (2 junior infant class) • Trawling questionnaire on cases for VTEC exposures • food, water, pets, travel, environmental (farms/cattle) • Cases screened GP/Paediatric Unit for HUS • Mapping of cases in relation to Group Water Scheme • Case control study
‘Outbreak Curve’ Symptomatic Asymptomatic Case definition: Living in West Limerick, stool E Coli 0157 VT2 +ve phage type 32, from October 2005.
Cases mapped to Group Water Scheme W=Well R=Reservoir Cluster 1 Group Water Scheme Cluster 2 Surrounding villages CASES Cluster 3
1st decision point – Friday October 28th • Friday pm before Bank Holiday weekend • Provisional positive results on 1 other child attending creche and 2 grandparents • Contacted • childminder to advise that service should cease until negative samples had been obtained from all children and the 2 childminders because of evidence of transmission within the childminding situationfamilies of remaining children to establish whether samples had been sent and to advise that creche would close • paediatric unit to arrange clinical follow-up • Childcare Unit to notify creche existence • GPs • EHOs- Co Council on standby for home water result • Lab- further samples • HPSC
3 further provisional positive results reported – 4 year old sibling at local primary school and 2 further children in creche OCT convened for November 2nd Primary school contacted during half-term break to arrange screening of junior infant class using school premises 2nd decision point Tuesday, November 1st 2005
3rd Decision point • On confirmation on Monday pm of 2 further provisional cases from Creche 2, both linked to GWS1, decision to contact Group Water Scheme trustees and Co. Council informed as a courtesy. • Positive response from Co. Council who arranged meeting for 8am 22/11/06 • Joint Boil Water notice distributed by Co. Council on same day • Grant provided by Co. Council towards disinfection upgrading
4th Decision point • Need to revisit descriptive epidemiology and consider further studies to outrule other common source of infection • Staffing crisis because of staff exhaustion over almost 4 weeks • Agreement with PCCC Ass/ Nat Director to second 3 AMOs to Public Health Dept and take over Incident Room to accommodate staff.( Not without protest!)
Case Control Study • ? continous common source • Hypotheses explored –childcare, water consumption, travel, farm exposure to cattle, pets and slurry, local meat suppliers, local food suppliers, functions/events/eateries attended. • Case definition:symptomatic case living in West Limerick who had stools positive for E. coli O157 VT2 + Phage type 32 • 3 controls per case, age group matched, same or adjoining PHN areas randomly selected from child databases • 36 participants (9 symptomatic cases/27 controls)
Other Investigations • Environmental sampling • Water samples-GWS, public supplies, private wells, • 1 food sample • Environmental inspections of schools, childcares, playgroup • Veterinary Investigation • Animal faeces near wells • Moores swab in water • Animal samples taken from 5 herds from cases with cattle and on farms adjacent to some wells on GWS • Home pasteurised milk from farm where 3 family cases
Microbiology-Faeces • >200 Faeces samples collected –Samples cultured for VTEC using pre-enrichment step • VT, phage type,antibiogram, PFGE • 167 contacts screened /152 contacts negative • 18 cases of E.coli O157 VT2+ve phage type 32 • One cattle sample positive for E. coli O157 VT2+ve phage type 32 • PFGE for all positive human and veterinary samples showed the same patterns
Microbiology-water • 59 Water samples/1 ham sample /home pasteurised milk • No VTEC in food/milk sample or water samples • House of case- E Coli 1/100ml, 26 coliforms • Raw water -E Coli 1/100 mls , 5 coliforms, 2 coliforms
Hydrogeology report on private Group Water Scheme (GWS) Vulnerable to contamination • Agricultural catchment area • Close contact wells/cattle • Limestone-surface seepage into ground water Problems with disinfection of 4 wells • constant vs. variable chlorination, • insufficient chlorine contact time, • flow in both directions • administrative
Control Measures • Hygiene advice to cases and contacts • “Voluntary” closure of two creches, junior infants class(<5 years) and playgroup • Exclusion of ‘at risk’ contacts/cases until microbiological clearance • Boil water notice on GWS( still in force!) • Improved chlorination of GWS • Education /monitoring/quality control of GWS • Communications • GPs, childcare centres • Media
Potential Problem areas • Consistency i.e. when to intervene and when to withold intervention • Staffing ( incl OOH) • Accommodation • Facilities – level 3 lab, fax etc • Communication – Log of events, email, etc • Relationships – PCCC ( difficult), Local Authority ( good), GPs ( good), vets( good) • Conflicting expert advice
Lessons • Significant person-to-person spread in child-minding and house-hold settings • Multiple risk factors in rural/agricultural area • Veterinary Perspective Need for a Programme of Routine Surveillance • Child care legislation - many child-minders are not notified to HSE • Poor public awareness re GWS • Training needs of GWS trustees • Need for category 3 containment level laboratory • Use of multidisciplinary/multi-agency OCT • Avoid Half term outbreaks!
Members of the OCT Dr. Tessa Greally Chair Mr. Denis Barron, Dr. Ann Carroll, Dr. Carmel Collins, Mr. Andy Curtin, Ms Annette Fitzgerald Dr. Rose Fitzgerald, Dr. Eleanor McNamara, Dr. Mai Mannix, Ms. Regina Monahan, Dr. Tom Norris, Dr. Nuala O’Connell, Dr. Fiona O’Dea, Dr. Mary O’Riordan, Dr. Terry Prendiville, Dr. Joe Quinn, Ms. Elaine Whelan, Mr. Dominic Whyte, Mr. Jim Buckley, Mr. John McCarthy, Dr. Paul McKeown, Other Acknowledgements Dr Tom Curtin Dr. Patricia Garvey Prof. Pat Wall Dr. Meirion Evans Dr. John Cowden Mr. Dick McMahon Mr. Tom Ward Mr. PJ Kelleher Mr. Cathal Ward Public Health Laboratory, HSE, Dublin Mid-Leinster Limerick County Council