Download
1 / 1
10 likes | 165 Views
Table 2. Separate conditional logistic regression models investigating the relationship between social support/network and case (DSH) status. A Case-control Study of the Association between Deliberate Self-harm and Prior Social Isolation.

E N D
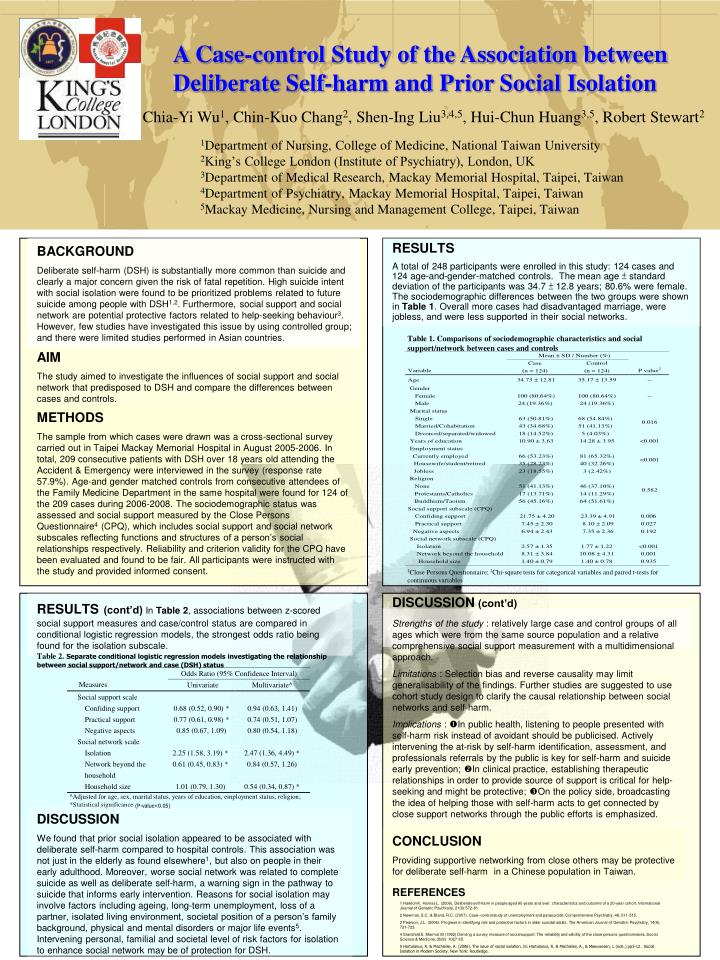
Table 2. Separate conditional logistic regression models investigating the relationship between social support/network and case (DSH) status A Case-control Study of the Association between Deliberate Self-harm and Prior Social Isolation Chia-Yi Wu1, Chin-Kuo Chang2, Shen-Ing Liu3,4,5, Hui-Chun Huang3,5, Robert Stewart2 1Department of Nursing, College of Medicine, National Taiwan University 2King’s College London (Institute of Psychiatry), London, UK 3Department of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan 4Department of Psychiatry, Mackay Memorial Hospital, Taipei, Taiwan 5Mackay Medicine, Nursing and Management College, Taipei, Taiwan BACKGROUND Deliberate self-harm (DSH) is substantially more common than suicide and clearly a major concern given the risk of fatal repetition. High suicide intent with social isolation were found to be prioritized problems related to future suicide among people with DSH1,2. Furthermore, social support and social network are potentialprotective factors related to help-seeking behaviour3. However, few studies have investigated this issueby using controlled group; and there were limited studies performedin Asian countries. RESULTS A total of 248 participants were enrolled in this study: 124 cases and 124 age-and-gender-matched controls. The mean age ± standard deviation of the participants was 34.7 ± 12.8 years; 80.6% were female. The sociodemographic differences between the two groups were shown in Table 1. Overall more cases had disadvantaged marriage, were jobless, and were less supported in their social networks. Table 1. Comparisons of sociodemographic characteristics and social support/network between cases and controls AIM The study aimed to investigate the influences of social support and social network that predisposed to DSH and compare the differences between cases and controls. METHODS The sample from which cases were drawn was a cross-sectional survey carried out in Taipei Mackay Memorial Hospital in August 2005-2006. In total, 209 consecutive patients with DSH over 18 years old attending the Accident & Emergency were interviewed in the survey (response rate 57.9%). Age-and gender matched controls from consecutive attendees of the Family Medicine Department in the same hospital were found for 124 of the 209 cases during 2006-2008. The sociodemographic status was assessed and social support measured by the Close Persons Questionnaire4 (CPQ), which includes social support and social network subscales reflecting functions and structures of a person’s social relationships respectively. Reliability and criterion validity for the CPQ have been evaluated and found to be fair. All participants were instructed with the study and provided informed consent. 1Close Persons Questionnaire; 2Chi-square tests for categorical variables and paired t-tests for continuous variables DISCUSSION(cont’d) Strengths of the study :relatively large case and control groups of all ages which were from the same source population and a relative comprehensive social support measurement with a multidimensional approach. Limitations : Selectionbias and reverse causality may limit generalisability of the findings. Further studies are suggested to use cohort study design to clarify the causal relationship between social networks and self-harm. Implications : In public health, listening to people presented with self-harm risk instead of avoidant should be publicised. Actively intervening the at-riskby self-harm identification, assessment,and professionals referrals by the public is key for self-harm and suicide early prevention; In clinical practice, establishing therapeutic relationships in order to provide source of support is criticalfor help-seeking and might be protective; On the policy side, broadcasting the idea of helping those with self-harm acts to get connected by close support networks through the public efforts is emphasized. RESULTS(cont’d)In Table 2, associations between z-scored social support measures and case/control status are compared in conditional logistic regression models, the strongest odds ratio being found for the isolation subscale. ^Adjusted for age, sex, marital status, years of education, employment status, religion; *Statistical significance (P-value<0.05) DISCUSSION We found that prior social isolation appeared to be associated with deliberate self-harmcompared to hospital controls. This association was not just in the elderly as found elsewhere1, but also on people in their early adulthood. Moreover, worse social network was related to complete suicide as well as deliberate self-harm, a warning sign in the pathway to suicide that informs early intervention. Reasons for social isolation may involve factors including ageing, long-term unemployment, loss of a partner, isolated living environment, societal position of a person’s family background, physical and mental disorders or major life events5. Intervening personal, familial and societal level of risk factors for isolation to enhance social network may be of protection for DSH. CONCLUSION Providing supportive networking from close others may be protective for deliberate self-harm in a Chinese population in Taiwan. REFERENCES 1 Hawton K. Harriss L. (2006). Deliberate self-harm in people aged 60 years and over: characteristics and outcome of a 20-year cohort. International Journal of Geriatric Psychiatry, 21(6):572-81. 2 Newman, S.C. & Bland, R.C. (2007). Case–control study of unemployment and parasuicide. Comprehensive Psychiatry, 48, 511-515. 3 Pearson, J.L. (2006). Progress in identifying risk and protective factors in older suicidal adults. The American Journal of Geriatric Psychiatry, 14(9), 721-723. 4 Stansfeld S, Marmot M (1992) Deriving a survey measure of social support: The reliability and validity of the close persons questionnaires. Social Science & Medicine, 35(8): 1027-35. 5 Hortulanus, R. & Machielse, A. (2006). The issue of social isolation. In: Hortulanus, R. & Machielse, A., & Meeuwesen, L (eds.) pp3-12 . Social Isolation in Modern Society. New York: Routledge.