Download

1 / 38
400 likes | 792 Views
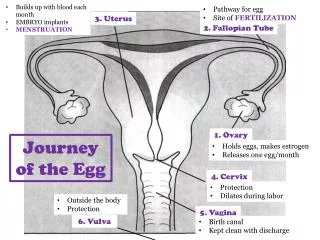
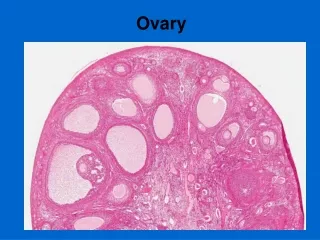
OVARY. Anatomy& Physiology The mature ovaries are paired nodular structures 2,5-5*2*1 cm The two major functions of the adult ovary: The synthesis and secretion of sex steroids The release of a mature ovum every 28-30days

E N D
Anatomy& Physiology The mature ovaries are paired nodular structures 2,5-5*2*1 cm The two major functions of the adult ovary: The synthesis and secretion of sex steroids The release of a mature ovum every 28-30days normally progress in concert with one another and are closely interrelated Physiology of the menstrual cycle
The Hypothalamic-Pituitary –Ovarian Axis The cyclic pulsatile frequency of GnRH secretion favors FSH or LH synthesis and secretion GnRH (+) (+) ESTRADIOL Gonadotroph cells FSH LH (-) (+) (+) (-) Granulosa cells Theca and stromal cells ESTRADIOL TESTOSTERONE INHIBIN ACTIVIN Corpus luteum PROGESTERONE
HORMONES OF THE OVARY → the mature ovary synthesizes and secretes estrogens, progesterone, androgen and their precursors The ovary is normally the major source of estrogens, although the conversion of androgens precursors in other tissues (eg adipose tissue) is clinically important after the menopause and in some women with disorders of ovarian function The ovary also produces and secretes large amounts of Pg during the luteal phase of the cycle It is also the source of small amounts of testosterone and other androgens : androstenedione that serve not only as precursors to estrogen synthesis ( the theca cells, which lack aromatase, under the influence of LH synthesize androgens; the androgens, mainly androstenedione diffuse into the granulosa cells ( which lack 17 hydroxylase )and are utilized for estrogen production← under the influence of aromatase expressed by these cells of ovarian follicle)but also are released into the circulation to act on peripheral tissues;
Physiologic effects of steroid hormones ►ovarian hormones-derived from cholesterol • ESTROGENS: 18 C → Estradiol (E2), Estrone (E1) - (+) the maturation of the vagina, uterus, uterine tubes at puberty as well as the secondary sex characteristics - (+) stromal development and ductal growth in the breast - are responsible for the acceleration of growth phase and the closing of the epiphyses of the long bones - alter the distribution of body fat so as to produce typical female contours, including some accumulation of body fat around the hips and breasts - role in development of the endometrial lining (proliferative phase) ( when estrogen production is properly coordinated with the production of Pg during the normal human menstrual cycle , regular periodic bleeding occur - Cervix :(+) production of large amounts of thin watery mucus, through which sperm can penetrate most readily PROGESTERONE: 19 C ← mainly by corpus luteum - (+) glandular development of the breasts - (+) cyclic glandular development of the endometrium (secretory phase) - ↑ the body temperature in humans - Cervix: ↓ mucus production and makes mucus thick ANDROGENS: 21 C → Testosterone, androstendione ovary, conversion in adipose tissue
Menstrual cycle LH Pg E2 FSH M M z.1 z.14 z.21 Folicullar phase Luteal phase
Evaluation of ovarian function I.DIRECT HORMONAL ASSESSMENT : plasma levels of FSH, LH, E2, Pg As a consequence of the changing rates of secretion of estrogens and progesterone throughout the menstrual cycle: • The basal functional status of the HPT-HPF-OVARIAN AXIS should be explored during early follicular phase(days:2-4):FSH, LH, E2 • The ovulation: during days :13-15 –the most common way is to detect the LH surge [measurement of urinary LH) (ovulation typically occurs 34-36 hours after the onset of the LH surge) [to predict that ovulation is going to occur] • Activity of corpus luteum - measurement of midluteal serum progesterone concentration (days:21-23) : - is used to document the occurrence of ovulation ( Pg>3ng/ml –indication that ovulation has occurred) - is used to assess a luteal phase defect ( Pg< 10 ng/ml suggests a luteal phase defect)
Evaluation of ovarian function • II. INDIRECT EVALUATION OF OVARIAN HORMONAL STATUS • A) the progestagen withdrawal testprovides a useful functional assessment of estrogenous status in women with a normal outflow tract ( see later) • B) measurement of basal body temperature throughout a cycle (BBT)=the simplest test to assess progesterone secretion
Ovarian failure (OF) • Classification of OF • -according to the site of the lesion • central • primary /peripheric • -according to the age at onset • before puberty • after puberty Partial ovarian failure (progesteronic, luteal phase defect) =ovulation with inadequate luteinization and↓Pg secretion during the luteal phase← result from disorders of gonadotropin secretion that cause poor follicular development and ↓ granulosa-cell growth → ↓ numbers of granulosa-lutein cells and ↓Pg secretion and ↓ endometrial maturation
PRIMARY OF Gonadal agenesis Gonadal dysgenesis (45 X: Turner’sdr and its variants) Iatrogenic (radiation, chemotherapy) Infecions (e.g mumps)) Autoimmune Resistant ovary sdr Defects in estrogen biosynthesis CENTRAL OF Hypothalamic etiology Lesions (organic) functional =hypothalamic amenorrhea stress Amenorrhea associated with eating disorders (anorexia nervosa, bulimia) Amenorrhea associated with strenuous exercise Pituitary etiology (see section HPT-HPF) Etiopathogenesis of OF
Clinical features in OF • OF WITH PREPUBERAL ONSET→poor sexual secondary sexual development and eunuchoid skeletal proportions • 1. SEXUAL INFANTILISM • Primary amenorrhea • Absence/sparse of pubic and axillary hair • Absence of breast development (telarcha) • Infantile aspect of external and internal genitalia • 2.SOMATIC MODIFICATIONS • Tall stature, eunuchoid skeletal proportions (crown to pubis to pubis to floor ratio<1) • Low peak bone mass • 3. PSYCHOLOGICAL DISTURBANCES • ↓ libido
Clinical features in OF • OF WITH POSTPUBERAL ONSET • Secondary amenorrhea • infertility • Decrease in axillary and pubic hair • Atrophy of breast • Involution of genital tract, urogenital atrophy →vaginal dryness and pain with intercourse, atrophic cystitis • Precocious appearance of wrinkles • Vasomotor symptoms (hot flushes) • complicatii tardive: osteoporosis, atherosclerosis, Alzheimer’s disease
Laboratory findings in primary amenorrhea (+ absence of sexual maturation)- ovarian failure with prepuberal onset • Hormonal assessment: FSH, LH, E2 • → ↓/ low-normal FSH, LH + ↓E2= secondary (central ) ovarian failure with prepuberal onset • In these patients, LH and FSH responses to testing with GnRH may help to differentiate delayed puberty from a more serious problem • do hormonal, neuroradiologic and neuro-ophatalmologic assessment of hypothalamus and pituitary ( e.g. tumors: craniopharyngiomas) • → ↑ FSH, LH + ↓ E2 =primary ovarian failure If the patient is short in stature and has obvious stigmas of Turner’s sdr → Barr test, Karyotype (45,X0) If the patient is of normal height or has relatively longer arms and legs compared with the length of the trunk( eunuchoid proportions) → search for other causes of primary ovarian failure: autoimmune ( do anti ovary autoantibodies), sonography, celioscopy with biopsy ( agenesis)
Laboratory findings in secondary amenorrhea (+ normal secondary sex characteristics)- ovarian failure with postpuberal onset • → localize the underlying cause of amenorrhea: dysfunction of either the outflow tract, the ovary, or the HPT-HPF • 1.! The possibility of pregnancy should always be considered ( pregnancy test!) • 2. serum PRL concentrations :→ ↑ PRL : search for a cause of hyperPRL: do TSH, FT4 ( to rule out a primary hypothyroidism), search for a prolactinoma/ “ dezinhibition” hyperPRL… • → PRL=normal → • 3. Assess endogenous estrogen (progesterone withdrawal test) The presence of endogenous estrogens can be established (by measuring E2 levels) or attempting to induce withdrawal uterine bleeding by adm. Progesterone: an oral progesterone- eg MPA 10 mg/day or duphastone 10-20mg/day dayly for 5-10 days test positive
Laboratory findings in secondary amenorrhea (+ normal secondary sex characteristics)- ovarian failure with postpuberal onset • Test negative =failure to induce menstrual bleeding by exogenous progestin indcates: • Insufficient estrogen production secondary to –hypothalamic-pituitary dysfunction - ovarian dysfunction 4. To differentiate them: Do gonadotropin level:FSH, LH, + E2 ↓/ low-normal FSH, LH + ↓ E2 = hypotalamic-pituitry disorder ↑ FSH, LH + ↓E2 = primary ovarian failure ! A normal response ( with bleeding) following treatment with a combination of estrogen +progestin (see next) is obtained- because the outflow tract is intact • Defect of the outflow tract with normal estrogen production ( an infrequent cause of secondary amenorrhea) 5. If one suspects this, its integrity can be assessed by administering an oral combination of estrogen+ progesterone ( CE for 21 days adding a progestin in the last5-10 days) - a lack of withdrawal bleeding following treatment usually indicates an abnormality of the outflow tract ( eg : Asherman’ s sdr← destruction of the endometrial cavity by chronic infections such as tuberculosis or destruction of the endometrium by curettage ; or Mullerian defects( Mayer-Rokitansky-Kuster-Hauser sdr= absence of the vagina with varying degrees of uterine development associated with normal ovarian function ( !!! Primary amenorrhea)
Treatment of OF • OF with prepuberal onset – replacement therapy to allow feminization • EE2 5 g/day increasing to 10-20 g/day depending upon the clinical results or conjugated estrogens (CE) 0.3-0.625mg/day on days 1-21 of the month; 10mg of medroxyprogesterone acetate (MPA) are then added on days 12-21 after physical signs of estrogen effect are noted and breakthrough bleeding occurs (and always within 6 months after initiating estrogen);!!! );later the patient may be switched to sequential oral contraceptives. If there is a coexisting GH deficiency (in the context of pituitary failure) first treat de GH deficiency, then add estrogen replacement therapy • OF with postpuberal onset – hormone replacement therapy (estrogens and progesterone ) in either a (cyclical) sequential regimen (0,625 mg of CE (or the equivalent doses of a variety of available products) days:1-25 of each month + 10mg of MPA for the last 10-14 days of every month) →withdrawal bleeding or continuous combined regimen: a combination of 0,625 mg of CE and 2,5mg of MPA is given orally every day → usually amenorrhea GnRH or FSH+ LH stimulation treatment if fertility is desired (in seconadry(central) ovarian failure) • Partial ovarian failure (progesteronic, luteal phase defect) :progesterone products –in the last 10days :days 16-25 • Medroxyprogesterone acetate (MEDROXIPROGESTERON) 5-10 mg/zi • didrogesteron (DUPHASTON) 10-20 mg/zi • mycronizat progesterone (UTROGESTAN) 100-300 mg/zi
Turner’s sdr ( syndrome of gonadal dysgeneis) • The classical form= 45, X0 karyotype represents 50% of all patients with X Cs abnormalities • Mosaicism : 45X0/46XX, 45X0/46XX/47XXX • Pathogenesis: a 45, X0 constitution may be a consequence of nondisjunction or chromosome (Cs) loss during gamethogenesis in either parent that result in a sperm or ovum lacking a sex Cs… • Clinical presentation: the cardinal features of 45, X0 gonadal dysgenesis are a variety of somatic anomalies, sexual infantilism at puberty secondary to gonadal dysgenesia and short stature I. Somatic anomalies I n infancy: lymphedema of the extremities Later in life: typical facies : micrognathia, a fish-like mouth with a narrow, high- arched palate epicantal folds, ptosis, strabism prominent, low-set, ears the neck is short, broad and the hairline in back is low; webbing of the neck the chest: usually square and shield-like, inverted nipples Additional anomalies: coarctation of the aorta, hypertension, renal abnormalities: rotation of the kidney, duplication of the renal pelvis and ureter ;pigmented nevi, cubitus valgus, short fourth metacarpals and metatarsals, scoliosis, reccurent otitis media
Turner’s sdr ( syndrome of gonadal dysgeneis) • II. Short stature Is an invariable feature of the syndrome; mean final height in 45, X0 patients is 143cm (mean:133-153 cm) ← ! Is not due to a deficiency of GH, IGF-I, sex steroids, or thyroid hormone ← [it is related, at least in part, to haploinsufficiency of the PHOG (psudoautosomal homeobox osteogenic gene)/SHOX (short stature homeobox gene) in the pseudoautosomal region of the X ] III. Gonadal dysgenesis The gonads : typically streak-like and usually contain only fibrous stroma The genital tract and external genitalia are female in charcter but immature Primary amenorrhea, sexual infantilism ← impaired ovarian function IV. Associated disorders: autommune thyroiditis, diabetes mellitus, inflammatory bowel disease
Laboratory findings • Hormonal evaluation FSH, LH↑ + ↓E2 X-ray findings:- shortening of the fourth metacarpal - knee: deformities of the medial tibial and femoral condyles with obliquely tipped tibial epiphyses and medial projections of the tibial metaphyses that can result in genu vallgum (Kosowicz’s sign) -scoliosis, osteoporosis Cardiac evaluation: echocardiogram ( for cardiovascular anomalies) IVU, renal sonogram: renal abnormalities Ultrasonography of the pelvis or MRI: rudimentary ovaries/ streak gonads small uterus Diagnosis Barr test ( determination of the X chromatin pattern (Barr body)- negative Karyotype analysis is the definitive procedure: 45,X0 / mosaicism
Treatment of Turner’ s sdr • → directed toward maximizing final height and inducing seconadry sexual characteristics and menarcha at an age commensurate with that of normal peers • Although the short stature is not due ←↓GH, administration of high-dose biosynthetic human GH result in an increase in final height • → give recombinant GH • → in patients who have been treated with GH and have achieved an acceptable height, estrogen replacement therapy is usually initiated after 12-13 years of age;… after the first year : add a progestin
Anatomy & structure-function relationship • The testes contain 2 major components which are structurally separated and serve different functions: • Leydig cells, or interstitial cells→testosterone (=the primary secretory product) → for embryonic differentiation along male lines of the external and internal genitalia → during puberty androgens mediate growth of scrotum, vas deferens, seminal vesicles, prostate, penis, (+) male secondary sexual development : skeletal growth and growth of the larynx, which results in deepening of voice, both ambisexual (pubic and axillary) hair growth and sexual (beard, mustache, chest, abdomen, and back) hair growth; (+) the epiphysial cartilaginous plates which results in the pubertal growth spurt → maintenance of libido and potency in the adult male
Anatomy & structure-function relationship • Seminiferous tubules ( =80-90% of the testicular mass) responsible for the production of spermatozoa during male reproductive life (puberty to death)-composed of: 1. Sertoli cells-functions: →Line the BM and form tight junctions with other Sertoli cells (these tight junctions prevent the passage of proteins from the interstitial space into the lumenus of the seminiferous tubules, thus establishinga “blood-testis barrier” →SecreteABP, a molecule with ↑ affinity for androgens; this substances, which enters the tubular lumen, provides a ↑concentration of testosterone to the developing germinal cells during the process of spermatogenesis. →FSH directly stimulates Sertoli cells to secreteinhibin and inhibin selectively (-) FSH release from the pituitary (reciprocal relationship) →Secrete antimullerian hormone(AMH)→ apoptosis of mullerian ducts 2.Germinal cells : SPERMATOGENESIS:spermatogonia→ I spermatocytes →II spermatocytes→spermatids →spermatozoa ! The interval from beginning of spermatogenesis to release of mature spermatozoa into the tubular lumen is 74 days
Seminiferous tubules – 80% Germinal cells LEYDIG CELLS – 20% Testosterone Anatomy • Sertoli cells • -androgen-binding protein (ABP) • -inhibin • - AMH
Hypothalamic-pituitary-testicular axis Pulsatile secretion GnRH (+) FSH LH (-) (+) (+) (-) ABP LEYDIG cells Germinal cells SPERMATOGENESIS TESTOSTERONE SERTOLI cells INHIBIN
CONTROL OF TESTICULAR FUNCTION • Hypothalamic-Pituitary-Leydig Cell Action GnRH( HPT) secreted in pulses every 90-120min → HPT-HPF-portal blood→ gonadotroph cells→ LH, FSH LH → Leydig cells→secretion of androgens In turn, ↑of androgens (-) LH from the anterior pituitary, througha direct action on the HPF and an inhibitory effect at the HPT level Hypothalamic-Pituitary –Seminiferous Tubular Axis GnRH → FSH → seminiferous tubules (Sertoli cells)→ ABP, inhibin FSH ↔ inhibin FSH is necessary for the initiation of spermatogenesis; however, full maturation of the spermatozoa appears to require not only an FSH effect but also testosterone.
MALE HYPOGONADISM (MH) • MH CLASSIFICATION • according to the site of the lesion • Central MH • primary / peripheryc MH • according to the age at onset • MH with prepuberal onset • MH with postpuberal onset
PRIMARY MH Bilateral anorchia (vanishing testes sdr) Defects in androgen biosynthesis (deficit of 17 α hydroxylase, 3β HSD deficiency) Defects in androgen action( complete androgen insensitivity-testicular feminization) Klinefelter’s sdr iatrogenic MH: trauma, radiation Viral orchitis Autoimmunity CENTRAL MH hypothalamic-pituitary disorders) Panhypopituitarism (tumors, infiltrations…) isolated LH and FSH deficiency with hyposmia or anosmia (Kallmann’s sdr) LH and FSH deficiency with complex neurologic sdr: Prader-Willi hyperprolactinemia Etiopathogenesis of MH
Clinical presentation • 1) androgen deficiency during the 2-3 rd months of fetal development→ varying degrees of ambiguity of the male genitalia and male pseudohermaphroditism • 2) androgen deficiency during the third trimester→ defects in testicular descent → cryptorhidism + micropenis • 3) prepubertal androgen deficiency→ poor secondary sexual development + eunuchoid skeletal proportions • SEXUAL INFANTILISM • testes remain small, the penis fail to enlarge, the scrotum does not develop the marked rugae characteristic of puberty • Absent or very sparse axillaery and pubic hair • Absent or very sparse facial, chest, upper abdominal and back hair • No erections • Inadequate spermatogenesis • SOMATIC CHANGES • Tall stature (or normal final height) with eunuchoid skeletal proportions (upper segment( crown to pubis) to lower segment( pubis to floor) ratio<1; similar because of the relatively greater growth in the upper extremities, the arm span of eunuchoid individuals exceeds height by 5 cm or more • Muscle mass does not develop fully, deposition of adipose tissue around the pelvic girdle • Low peak bone mass • the voice remain high-pitched • Pale skin, and precocious appearance of wrinkles • Psychological disturbances • ↓ libidou
Clinical presentation • MH with postpuberal onset • Atrophy of the testes → small testes with a mushy or soft consistency • Atrophy of prostate • Erectile dysfunction, ↓ libidou • Spermatogenesis disturbances • Infertility • Absent or diminishing of facial hair (frequency of shaving ↓) and thoracic hair • ↓→0 of axillary and pubic hair • gynecomastia • Muscle hypotrophy and excess deposition of adipose tissue around the pelvic girdle • Pale skin+ fine wrinkles may appear in the corners of the mouth and eyes and together with the sparse beard growth → classic hypogonadal facies • Osteoporosis, atherosclerosis, fatigue • +/- hot flushes
Evaluation of Male Hypogonadism • HORMONAL ASSESSMENT: Gonadotropin and steroid measurement –basal determination and dynamic tests LH, FSH-the primary use of basal FSH, LH concentrations is to distinguish between hypergonadotropic hypogonadism (primary gonadal failure) and hypogonadotropic hypogonadism (secondary gonadal failure) → LH, FSH –low-normal/ ↓ + ↓ T (testosterone) = hypogonadotropic hypogonadism →! Serum PRL measurement → further evaluation of anterior and posterior pituitary gland function with appropriate pituitary function tests + neuroradiologic and neuro-ophtalmologic studies Dynamic test : GnRH test : assess the functional integrity of the gonadotroph tissue → Do FSH, LH at 0’ and 30’ after adm. of 100ug of GnRH iv. In normal men → LH ↑ 4-5 * basal levels while FSH ↑2* basal values Patients with destructive lesion of the pituitary and those with long-standing hypogonadism due to hypothalamic disorders ( secondary hypogonadism): no response/ partial response
Evaluation of Male Hypogonadism • → ↑ LH, FSH + ↓ T= hypergonadotropic hypogonadism( primary testicular disease) • → chromosomal analysis → differentiate between genetic abnormalities (XXY or variants) acquired testicular defects Dynamic test: h CG stimulation test To assess Leydig function before puberty, it is common to measure the response of plasma T to gonadotropin stimulation as an index of Leydig cell reserve . Human chorionic gonadotropin (h CG) – biologic actions similar to those of LH ( (+) the synthesis and secretion of testicular steroids in Leydig cells) Do T before and 72 h and 96 h after a single im dose of hCG (5000ui in adults or 100UI/kg in children) → a normal response: a doubling of the T level → in primary gonadal disease: 0/↓ response Useful : for differentiation between anorchia and cryptorchidism → anorchia : no response → cryptorchidism: T will rise
Evaluation of Male Hypogonadism • SEMEN ANALYSIS • TESTICULAR BIOPSY
MH treatment • = replacement treatment • the aim is to restore or normalize male secondary sexual characteristics and male sexual behavior and to promote normal male somatic development • DRUGS: • TESTOSTERONE ENANTHATE or CYPIONATE im 200mg every 2 weeks; • TESTOSTERONE UNDECANOAT (NEBIDO) 1000mg every 3 months • Transdermal testosterone patches: daily application • TESTOSTERONE GEL (ANDROGEL) 50mg daily ! !! In hypogonadal boys : institute androgen therapy between the ages 12-14 years ! In patients with hypogonadism due to inadequate gonadotropin secretio, spermatogrnesis (and virilization) may be induced by exogenous gonadotropin injections (hCG, FSH)
Klinefelter’s syndrome (XXY seminiferous dysgenesis) • =the most common development defect of the testis • The underlying defect is the presence of an extrs X Cz, the usual chromosomal karyotype being either 47XXY (classic form) or 46, XY/47, XXY (mosaic form) • Pathophysiology • The XXY genotype is usually due to maternal meiotic nondisjunction → an egg with two X Cs ( ! The frequency of meiotic errors correlates positively with maternal age) • Histologic changes in the testes:hyalinization and fibrosis of the tubules, absence of spermatogenesis (← obliteration of the seminiferous tubules) Leydig cells are also abnormal
Klinefelter’s syndrome • CLINICAL FEATURES - mean body height ↑←longer lower body segment; abnormal skeletal proportions that are not truly eunuchoid ( pubis-to-floor height is greater than crown-to-pubis height but span is less than total height) ! Is not secondary to androgen deficiency but is probably related to the underlying chromosomal abnormality -Gynecomastia -↓facial hair, axillary hair -Testes are small (<2 cm in longest axis, and 4ml in volume) and firm -Penis and scrotum ( during puberty) undergo varying degrees of development, with some individuals appearing normal! -Infertility, ↓libidou and potency -Learning disabilities, intellectual impairement and poor impulse control - feeling of inadequacy, dyssocial behaviour - osteoporosis
Klinefelter’s syndrome • LABORATORY FINDINGS • Semen analysis: Azoospermia • T↓, ↑FSH (especially) ,↑LH • The buccal smear is chromatin-positive (>20% of cells having a Barr body) • Chromosomal analysis → 47, XXY karyotype • Testicular biopsy: hyalinization of the seminiferous tubules, severe deficiency of spermatogonia • TREATMENT → directed toward androgen replacement therapy