Download
1 / 50
500 likes | 580 Views
Ovary. Dr. Amitabha Basu MD. Topic. Normal ovary Polycystic ovary Tumors of the ovary. Normal ovary gross. Micro. Th) Theca (MG) Membrana granulosa (CR) Corona radiata (ZP) Zona pellucida (CL) Corpus luteum. Polycystic ovarian disease. Definition Morphology Clinical features.

E N D
Ovary Dr. Amitabha Basu MD
Topic • Normal ovary • Polycystic ovary • Tumors of the ovary
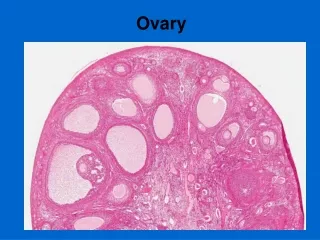
Micro Th) Theca (MG) Membrana granulosa (CR) Corona radiata (ZP) Zona pellucida (CL) Corpus luteum
Polycystic ovarian disease • Definition • Morphology • Clinical features
Pathophysiology • Excessive secretion of estrogen and androgen. • High LH • Low FSH • LH/FSH Ratio: high
Clinical features/complications • Oligomenorrhoea (Polycystic ovarian disease with oligomenorrhea is known as Stein-Leventhal syndrome) • Hirsuitism • Infertility • Endometrial Hyperplasia.
Classification Subtypes Age Incidence Etiopathogenesis Serous tumors Mucinous tumors Dysgerminoma Teratoma Granulosa-theca cell tumor Sertoli Leydig cell tumor Metastasic tumor Tumors of the Ovary
Classification • Tumor arising form the surface epithelium • Tumor arising form the germ cells • Tumor arising form Sex-cord stroma surface epithelium • Metastasic tumor
Multiparty Family history Genes BRCA 1 AND BRCA 2 ( IN HEREDITARY OVARIAN CANCER) ERB B2 K-RAS TP53 Etiopathogenesis
Serous tumor : Types • Benign • Borderline • Malignant Note: All surface epithelial tumors can be divided in these three types
Features of Serous tumor • Common ovarian tumor. • Mostly benign. • Cysts are lined by single Ciliated columnar epithelium. • Cyst contain serous fluid. • Bilateral (25%) • Usually Small.
Microscopy of serus tumor: Cysts are lined by single Ciliated columnar epithelium
Borderline Serous Tumor • Between benign cyst adenomas and malignant cystadenocarcinomas lies the grey zone of "borderline" lesions that are not clearly malignant, but are treated as though they could be.
Malignant serous Tumor : Papillary serous cystadenocarcinomas : note papillary areas.
Microscopy : Papillary process and cellular crowding and Psammoma body (not seen)
Spread of the tumor • These neoplasms characteristically spread by "seeding" along peritoneal surfaces. • Marker for Surface epithelial tumors: CA 125
Features of Mucinous tumor • Not common ( 10%), Large • Cysts are lined by single layer Mucin secreting columnar epithelium. • Cyst contain Mucinous gelatinous fluid: if rupture produce Pseudomyxoma peritonei.
Histology : Multilocular cysts lined by a single layer of benign mucinous columnar epithelium.
Teratoma • Types • Dermoid cyst • Immature malignant Teratoma • Struma Ovarii.
Types • Benign Teratoma ( Mature: usually cystic) • Malignant Teratoma( Immature : usually solid) • Monodermal Teratoma ( carcinoid Tumor, struma ovarii)
Benign Teratoma ( Mature)of ovary • It is also called Dermoid cyst. ( because it contains dermal appendages).
Immature Malignant Teratoma • Mean age : 18 years • Features : bulky, solid • Histology : Tissue containing immature neural tissue with neuroepithelial differentiation.
Dysgerminoma • Etiopathogenesis : Occur with gonadal dygenesis. • Radiosensitive tumor : 80% cure • Unilateral
Granulosa-theca cell tumor • Age : Post menopause but any age • Unilateral • Diagnostic point : Presence of call Exner body in Histology. • Function: Secrete estrogen ; promote endometrial, breast carcinoma.
Sertoli Leydig cell tumor • Age: all age • Unilateral • Point for identification: Gross: Yellow brown, solid. Micro: Pink Sertoli Leydig cells. • Clinical effect: Masculinizing ( defeminizing).
Struma ovarii • In this tumor the Teratoma contain predominantly thyroid tissue.
Metastasic tumor • Age: older age • Primary Tumor: Breast, lung, GIT • Big bilateral mass • Example : Tumor name : Krukenberg tumor
Krukenberg tumor • Primary tumor : Gastric adenocarcinoma • Route of metastasis : Seeding through body cavity. • Bilateral always. • Histology : contain “ signet ring” cells.
Nice to Know this Tumor: Thecoma-fibroma • Any age • Unilateral • Produce Meigs syndrome( ovarian tumor with ascites and Hydrothorax)
Review • Endometriosis ( clinical features) • Endometrial Hyperplasia . Etiology with C/F • Dermoid cyst Gross identification. • Leiomyoma identification and c/f • Carcinoma in situ • Granulosa theca cell tumor.
Review • Metastasic tumors • Ectopic pregnancy • Genes for Ovarian cancers. • Clear cell carcinoma • Vaginitis • Lichen sclerosus • Polycystic ovary • Gonorrhea infection (PID) • Anovulatory cycle : and other Causes of DUB