Download
1 / 19
190 likes | 330 Views
Bivalirudin Monotherapy Improves 30-day Clinical Outcomes in Diabetics with Acute Coronary Syndrome: Report from the ACUITY Trial. Frederick Feit, Steven Manoukian, Ramin Ebrahimi, Charles Pollack, Magnus Ohman, Michael Attubato, Roxana Mehran and Gregg Stone.

E N D
Bivalirudin Monotherapy Improves 30-day Clinical Outcomes in Diabetics with Acute Coronary Syndrome: Report from the ACUITY Trial Frederick Feit, Steven Manoukian, Ramin Ebrahimi, Charles Pollack, Magnus Ohman, Michael Attubato, Roxana Mehran and Gregg Stone
Bivalirudin Monotherapy Improves 30-day Clinical Outcomes in Diabetics with Acute Coronary Syndrome: Report from the ACUITY Trial Conflicts: Shareholder: Johnson and Johnson, Medicines Co., Millenium Pharmaceuticals; Consultant: Medicines Co.
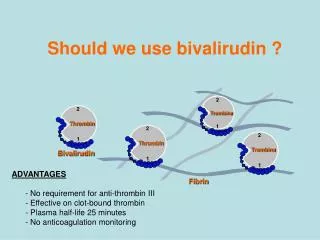
ACS in Diabetics: Metabolic Abnormalities • Increased blood glucose causes coronary artery inflammation and is prothrombotic • Increased generation of thrombin, CRP, fibrinogen, von Willebrand factor, factors VII and VIII, and platelet factor 4 • Increased expression of platelet activation markers including p-selectin, which mediates platelet-leukocyte interactions • Higher proportion of platelets expressing GPIIb/IIIa receptors
ACS in Diabetics: Background • Based on prior data including a meta-analysis of ACS trials current clinical guidelines recommend the use of GPIIb/IIIa inhibitors (GPI) in diabetic patients with ACS, especially those in whom PCI is planned1 • In the ACUITY Trial 13,819 pts, including 3852 diabetics, with moderate or high risk ACS, undergoing an early invasive strategy were randomly assigned to either the standard of care: Heparin (UFH or enoxaparin) + GPI; or, Bivalirudin + GPI; or Bivalirudin with provisional GPI 1. Roffi et al. Circulation.2001;104:2767-71
ACS in Diabetics: Methods • We compared adverse events: composite ischemia (death, nonfatal MI, unplanned ischemia driven revascularization), major bleeding and net clinical outcome (composite ischemia or bleeding) within the first 30 days in diabetic vs. nondiabetic pts • We compared the same 30-day end points in diabetic pts by treatment group
ACUITY Design ACS: Unstable angina or NSTEMI, N=13,819 Chest pain >10’ within 24 hours, plus Biomarker +, or Dynamic ECG changes, or Documented CAD or all other TIMI risk criteria ASA Clopidogrel per local practice Prior UFH, LMWH (1 dose), eptifibatide and tirofiban allowed Bivalirudin + IIb/IIIa inhibitor Bivalirudin + provisional IIb/IIIa Enoxaparin or UFH + IIb/IIIa inhibitor Cath within 72 hours PCI, CABG or medical management 30 day endpoints Death, MI, IUR, ACUITY major bleeding (net clinical outcome) Stone et al. Presented 2006; ACC
Study Medications • Anti-thrombin agents (started pre angiography) 1 Target aPTT 50-75 seconds 2 If last enoxaparin dose ≥8h - <16h before PCI; 3 If maintenance dose discontinued or ≥16h from last dose 4 Discontinued at end of PCI with option to continue at 0.25mg/kg for 4-12h if IIb/IIIa inhibitor not used 5 Bivalirudin option for off-pump same as PCI dose. For on-pump bivalirudin discontinued 2 hours before 6 Option to continue with pre-PCI anti-thrombotic regimen at physician discretion
ACS in Diabetics: Angiographic Triage * - p<0.001
ACS in Diabetics: Baseline Characteristics * CrCL <60 mL/min
ACS in Diabetics: 30-Day Outcomes Diabetes vs. No Diabetes P = 0.0002 P = 0.0037 P = 0.0002 †Heparin=unfractionated or enoxaparin
Diabetic ACS Patients Baseline Characteristics by Treatment * creatinine clearance <60 mL/min †Heparin = unfractionated or enoxaparin
P = 0.94 P = 0.64 P = 0.43 Diabetic ACS Patients: 30-Day Endpoints by Treatment Group Heparin* + GP IIb/IIIa vs. Bivalirudin + GP IIb/IIIa *Heparin = unfractionated or enoxaparin
P = 0.02 P = 0.39 P=0.0002 Diabetic ACS Patients: 30-Day Endpoints Heparin* + GP IIb/IIIa vs. Bivalirudin alone *Heparin = unfractionated or enoxaparin
P = 0.39 P = 0.32 P= 0.27 P = 0.37 Diabetic ACS Patients: Components of Ischemic Endpoint Heparin* + IIb/IIIa vs. Bivalirudin Alone *Heparin=unfractionated or enoxaparin
Diabetic ACS Patients: Myocardial Infarction Classification* Heparin† + IIb/IIIa vs. Bivalirudin Alone p = 0.27 5.6% 4.7% 30 day events (%) Q-wave 1.6% p = 0.05 Q-wave 0.8% Non Q-wave Non Q-wave p = 0.87 3.9% 4.0% Heparin + IIb/IIIa Bivalirudin alone (N=1298) (N=1287) *CEC-adjudicated †Heparin=unfractionated or enoxaparin
Diabetic ACS Patients: Bleeding Endpoints 30-days *P value for bivalirudin alone vs. heparin + IIb/IIIa inhibitor †Heparin=unfractionated or enoxaparin
Insulin-dependent Diabetic ACS Patients: 30-Day Endpoints by Treatment Group Heparin† + GP IIb/IIIa vs. Bivalirudin alone P = 0.23 P = 0.74 P = 0.04 †Heparin=unfractionated or enoxaparin
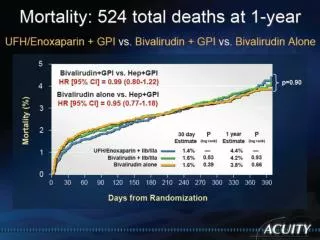
Diabetic Patients with ACS : Conclusions • Compared with non-diabetics, diabetic patients have worse net clinical outcomes at 30 days (12.8% vs. 10.5%; p=0.0002), resulting from significantly higher rates of the composite ischemic end point (8.6% vs. 7.2%; p=0.0037) and non-CABG major bleeding (5.7% vs. 4.2%; p=0.0002) • In diabetic patients, compared with the standard of care, heparin (UFH or enoxaparin) + GPIIb/IIIa, bivalirudin + GPIIb/IIIa was not better for protection from ischemic events or bleeding and resulted in similar net clinical outcome
Diabetic Patients with ACS: Conclusions • Compared to those receiving the reference standard, diabetics receiving bivalirudin monotherapy, with provisional GPIIb/IIIa in 7.9%, had similar protection from ischemic events (7.8% vs. 8.8%; p=0.39) and a marked reduction in major bleeding (3.7% vs. 7.1%; p=0.0002) with improved net clinical outcome (10.8% vs. 13.7%; p=0.02) • These 30-day outcomes suggest that bivalirudin monotherapy is safe and effective for diabetic patients with ACS, including those requiring insulin • One-year clinical and economic data will determine whether this regimen will become the standard of care for these patients.