Download
1 / 31
341 likes | 857 Views
Kidney and Urinalysis. Prepared by: Sr. Siti Norhaiza Hadzir. Functions of the kidney. Elimination of excess body water Elimination of waste products of metabolism e.g urea & creatinine Elimination of foreign substances e.g drugs

E N D
Kidney and Urinalysis Prepared by: Sr. Siti Norhaiza Hadzir
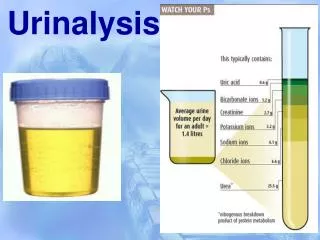
Functions of the kidney • Elimination of excess body water • Elimination of waste products of metabolism e.g urea & creatinine • Elimination of foreign substances e.g drugs • Retention of substances necessary for normal body function e.g protein, amino acids & glucose • Regulation of electrolytes balance & osmotic pressure of the body fluids.
The Nephron • The functional unit of the kidney. • Consists of renal corpuscle (glomerulus) & renal tubule. • Structure of glomerulus • Structure of tubule
Kidney blood supply • Renal artery from aorta → afferent arterioles → efferent arterioles → renal vein → heart
Glomerular Filtration Rate • Normally this amounts to about 130mL per minute (180 liters per 24 hours).
Renal Function Test • Falls into 2 major group: • Detect the presence of disease- not give indication as to the degree of functional impairment e.g proteinuria, cast, hematuria, WBC • Evaluate the degree of impairment e.g BUN, creatinine
Test of Urinary tract involvement • Healthy glomerular permeable membrane passes only substances with MW of less than 70 000. • Excess small proteins are reabsorbed completely by proximal tubule • Albumin is very close to cut off value (70000MW) can get access to the urine in glomerular disease. • Proteinuria are classified into 3: • Pre-renal- The glomerular membrane damage and tubular reabsorption inefficiency e.g Bence Jones protein in multiple myeloma. • Renal- renal parenchyma disease e.g amyloidosis. • Postrenal- Urinary tract problem e.g inflammation • Proteinuria
Figure 1: Normal urine is compared with proteinuria sample. Note increase in turbidity in proteinuria sample
Cast • Cast are precipitates of protein formed in the distal convoluted and collecting tubules of the kidney, where conditions of filtrate flow and pH are optimal for protein precipitation. • Normal condition-hyaline cast in small number • Large number indicates active renal disease.
Nature of cast • It is a muco-protein formed normally by the tubule; it is not formed in plasma. • It is long, rod like, flexible molecule. • As the glomerular filtrate travels down the nephron tubule, the concentrations of salts & H+↑. • At pH about 4.5, albumin and myoglobin change from negatively to positively charge molecules, the muco-protein is still negatively charge. • Opposite electric charge leads to precipitation and the formation of casts.
Hematuria & hemoglobinuria • Presence indicate bleeding within the urinary tract. • In acute glomerulonephritis there is hemorrhage from the glomeruli, Hb is convreted to hematin and methemoglobin. • These factors combine to give the “smoky” red brown urine characteristic of the disease.
Figure 2: The presence of blood in the urine
White Blood Cells • An increased number of white blood cells in a correctly collected specimen indicates inflammation in the urinary tract.
Test for Degree of Renal Impairment • Test based on water elimination and reabsorption • Blood Urea Nitrogen (BUN) • Creatinine • BUN: Creatinine
Test based on water elimination and reabsorption • Normally, conservation of water is reflected by concentrated urine with a high specific gravity • Excretion of an excess of water is illustrated by urine of low specific gravity
Impaired concentrating power • Tubular damage e.g chronic glomerulonephritis, polycystic disease • Severe potassium depletion • Hypercalcemia e.g due to vitamin D intoxication, hyperPTH • Inborn defects of tubular function • Diabetes insipidus
Non-protein nitrogen in blood • It is heterogenous collection of substances including urea, creatinine, uric acid, nucleotides, glutathione. • Estimation of NPN was replaced by determination of urea and creatinine, more specific indicators of renal condition, easily automated.
Blood Urea/BUN • Urea is the major excretion product of protein catabolism. • After elaboration, urea is passed to the blood and is excreted through the glomeruli and partly reabsorbed in the tubules.
Causes of ↑ BUN • Pre-renal: Circulation in the kidney is less efficient e.g CCF • Renal: Renal parenchyma damage, phylonephritis • Post-renal: Obstruction to the urinary tract • Presence of high level of urea is called uremia. • Very high level of urea leads to azotemia with kidney failure.
Creatinine • Nitrogenous substances found in muscle. • Since creatinine is derived entirely from endogenous metabolism (not form dietary protein) and is not reabsorbed by the renal tubules, its blood level; is a reliable index to renal function.
BUN/creatinine ratio • Normal ratio is 10:1. • Ratio more than 10:1 occur in: • Ration less than 10:1 occur in: • Excessive turnover of protein (hemorrhage, burns and infection) • Reduced glomerular perfusion • Repeated dialysis • Severe vomiting or diarrhea • Liver failure
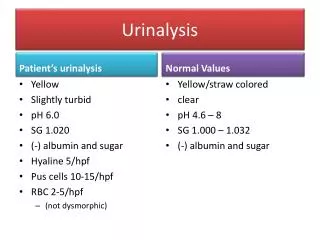
Routine urinalysis • The procedure • Urine collection and storage • Macroscopic examination • - Color • - turbidity and clarity (smoky. milky, cloudy) • - smell • - SG and osmolality
Urine container Centrifuge tube Pipetting the supernatant
The procedure: cont; • Urine processing • Centrifuge • Separate debris and supernatant • Microscopic examination [cells (epithelium, RBC, • WBC, cast, mucus tread, ova and parasites, • crystals] • Biochemical analysis (pH, protein, glucose, ketones, bilirubin, blood, nitrite, urobinogen, ascorbic acid)