Download
1 / 1
10 likes | 140 Views
An Obsessive Fascination for an Obstetric Physician Sivanathan J (1), Rajendran JA (1), Puvanandran D (2), Palaniappan K (1 ), Jegasothy R (1) (1) Hospital Kuala Lumpur; (2) Ministry of Health, Malaysia. Methods. Results. Objectives. Conclusions.

E N D
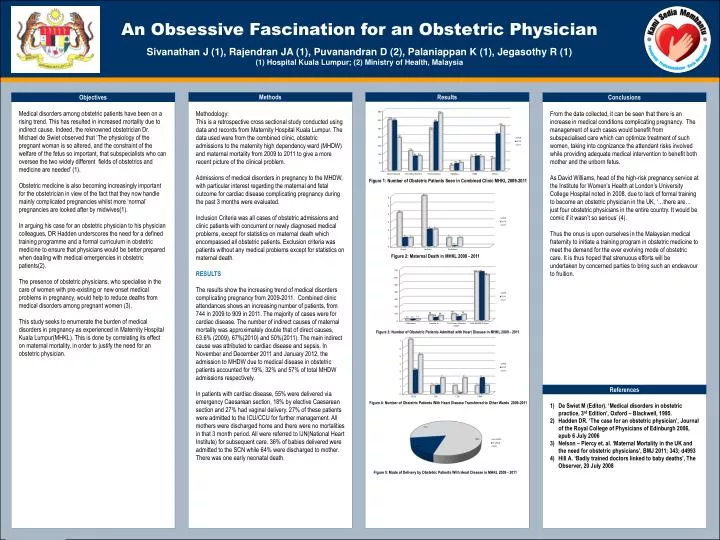
An Obsessive Fascination for an Obstetric Physician Sivanathan J (1), Rajendran JA (1), Puvanandran D (2), Palaniappan K (1), JegasothyR (1)(1) Hospital Kuala Lumpur; (2) Ministry of Health, Malaysia Methods Results Objectives Conclusions Medical disorders among obstetric patients have been on a rising trend. This has resulted in increased mortality due to indirect cause. Indeed, the reknowned obstetrician Dr. Michael de Swiet observed that ‘The physiology of the pregnant woman is so altered, and the constraint of the welfare of the fetus so important, that subspecialists who can oversee the two widely different fields of obstetrics and medicine are needed’ (1). Obstetric medicine is also becoming increasingly important for the obstetrician in view of the fact that they now handle mainly complicated pregnancies whilst more ‘normal’ pregnancies are looked after by midwives(1). In arguing his case for an obstetric physician to his physician colleagues, DR Hadden underscores the need for a defined training programme and a formal curriculum in obstetric medicine to ensure that physicians would be better prepared when dealing with medical emergencies in obstetric patients(2). The presence of obstetric physicians, who specialise in the care of women with pre-existing or new onset medical problems in pregnancy, would help to reduce deaths from medical disorders among pregnant women (3). This study seeks to enumerate the burden of medical disorders in pregnancy as experienced in Maternity Hospital Kuala Lumpur(MHKL). This is done by correlating its effect on maternal mortality, in order to justify the need for an obstetric physician. Methodology: This is a retrospective cross sectional study conducted using data and records from Maternity Hospital Kuala Lumpur. The data used were from the combined clinic, obstetric admissions to the maternity high dependency ward (MHDW) and maternal mortality from 2009 to 2011 to give a more recent picture of the clinical problem. Admissions of medical disorders in pregnancy to the MHDW, with particular interest regarding the maternal and fetal outcome for cardiac disease complicating pregnancy during the past 3 months were evaluated. Inclusion Criteria was all cases of obstetric admissions and clinic patients with concurrent or newly diagnosed medical problems, except for statistics on maternal death which encompassed all obstetric patients. Exclusion criteria was patients without any medical problems except for statistics on maternal death. RESULTS The results show the increasing trend of medical disorders complicating pregnancy from 2009-2011. Combined clinic attendances shows an increasing number of patients, from 744 in 2009 to 909 in 2011. The majority of cases were for cardiac disease. The number of indirect causes of maternal mortality was approximately double that of direct causes, 63.6% (2009), 67%(2010) and 50%(2011). The main indirect cause was attributed to cardiac disease and sepsis. In November and December 2011 and January 2012, the admission to MHDW due to medical disease in obstetric patients accounted for 19%, 32% and 57% of total MHDW admissions respectively. In patients with cardiac disease, 55% were delivered via emergency Caesarean section, 18% by elective Caesarean section and 27% had vaginal delivery. 27% of these patients were admitted to the ICU/CCU for further management. All mothers were discharged home and there were no mortalities in that 3 month period. All were referred to IJN(National Heart Institute) for subsequent care. 36% of babies delivered were admitted to the SCN while 64% were discharged to mother. There was one early neonatal death. From the data collected, it can be seen that there is an increase in medical conditions complicating pregnancy. The management of such cases would benefit from subspecialised care which can optimize treatment of such women, taking into cognizance the attendant risks involved while providing adequate medical intervention to benefit both mother and the unborn fetus. As David Williams, head of the high-risk pregnancy service at the Institute for Women’s Health at London’s University College Hospital noted in 2008, due to lack of formal training to become an obstetric physician in the UK, ‘…there are… just four obstetric physicians in the entire country. It would be comic if it wasn’t so serious’ (4). Thus the onus is upon ourselves in the Malaysian medical fraternity to initiate a training program in obstetric medicine to meet the demand for the ever evolving mode of obstetric care. It is thus hoped that strenuous efforts will be undertaken by concerned parties to bring such an endeavour to fruition. Figure 1: Number of Obstetric Patients Seen in Combined Clinic MHKL 2009-2011 Figure 2: Maternal Death in MHKL 2009 - 2011 Figure 3: Number of Obstetric Patients Admitted with Heart Disease in MHKL 2009 - 2011 References De Swiet M (Editor). ‘Medical disorders in obstetric practice, 3rd Edition’, Oxford – Blackwell, 1995. Hadden DR. ‘The case for an obstetric physician’, Journal of the Royal College of Physicians of Edinburgh 2006, epub6 July 2006 Nelson – Piercy et. al. ‘Maternal Mortality in the UK and the need for obstetric physicians’, BMJ 2011; 343; d4993 Hill A. ‘Badly trained doctors linked to baby deaths’, The Observer, 20 July 2008 Figure 4: Number of Obstetric Patients With Heart Disease Transferred to Other Wards 2009-2011 Figure 5: Mode of Delivery by Obstetric Patients With Heart Disease in MHKL 2009 - 2011