Download
1 / 18
180 likes | 316 Views
Treatment of Comorbid Depression and Alcohol Use Disorders. An Evidence-Based Approach Abby L. Goldstein, Ph.D. The Clinical Scenario. 34 year old Caucasian woman presents with history of MDD, first episode in college, but no formal treatment Currently meets criteria for MDE

E N D
Treatment of Comorbid Depression and Alcohol Use Disorders An Evidence-Based Approach Abby L. Goldstein, Ph.D.
The Clinical Scenario • 34 year old Caucasian woman presents with history of MDD, first episode in college, but no formal treatment • Currently meets criteria for MDE • During clinical interview, she reveals she is consuming 3-4 glasses of wine per day • Started drinking in the past three months • Has had 2 prior depressive episodes – this is the first episode in which drinking is concurrent • She is concerned about her depression, but does not feel her drinking is a problem • Upon further inquiry, she notes that her husband has asked her to cut-down her drinking and that she drinks because it helps her “feel better”
The Question How would you proceed with treating this patient?
Clinical Questions • Does she meet DSM-IV criteria for alcohol abuse? Is this “at-risk” drinking? • Are antidepressants appropriate for comorbid alcohol abuse and MDD? • Is psychotherapy appropriate? • Should depression be treated in the context of alcohol abuse/use?
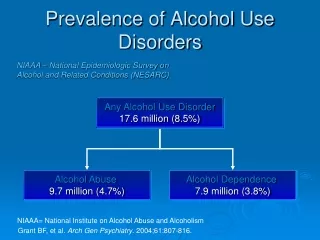
The Prevalence of AUDs Among Individuals with MDD • Estimates of AUD diagnosis among individuals with MDD • 21% current AUD diagnosis among community sample with MDD (Grant & Hartford, 1995) • 9% current AUD diagnosis among psychiatric sample (Salloum et al., 1995) • Lifetime estimates range from 30% to 40%
Outcomes Associated with Comorbid Depression and AUDs • Comorbidity associated with: • Higher rates of divorce and living alone (Sullivan, Fiellen, & O’Connor, 2005) • Persistent depression increases risk of relapse, AUD prolongs course of depression, and comorbidity associated with greater utilization of health care resources (Pettinati, 2004) • Increased risk of suicide (e.g., Conner & Duberstein, 2004)
DSM-IV Substance Abuse(APA, 1994) • Pattern of substance use leading to clinically significant impairment or distress • One or more consequences within 12 months • Failure to fulfill major role obligations • Use in physically hazardous situations • Recurrent substance-related legal problems • Continued use despite persistent social or interpersonal problems • Symptoms have not met criteria for dependence for this class of substances
Diagnosing Alcohol Abuse • No specific quantity/frequency criteria for DSM-IV diagnosis of alcohol abuse • NIAAA criteria for “at-risk drinking” • Men >14 drinks per week or >4 drinks per occasion • Women >7 drinks per week or >3 drinks per occasion
Practice Guidelines • UMHS guidelines for depression treatment includes AUDs in the following ways: • Alcohol abuse identified as a risk factor for depression • DO NOT USE • Cymbalta if concurrent heavy alcohol use • Wellbutrin if history of substance abuse (does not specify alcohol versus other) • Ask CAGE questions • Special Rx Considerations: • Address alcohol use to attempt to achieve period of sobriety • If unable to achieve sobriety, treat with SSRI • Be vigilant in assessing suicidal risk
Searching the Literature • UM-MEDSEARCH • Database: All EBM Reviews • Alcohol and (abuse or dependence) - 1573 • Major depression - 2235 • Antidepressant Medication - 314 • Combine: 28 • Database: Ovid Medline • Limit: EBM Reviews • Alcohol$ and depress$ and treatment • 44 Hits – 3 recent reviews on treatment of depression and substance abuse disorders • 1 identified as meeting CRD criteria and reviewed • PSYCINFO • Several additional reviews
Reviewing the EvidenceTorrens, Fonseca, Mateu, & Farre (2005) • Systematic review and meta-analysis of SUDs with and without comorbid depression • Only included randomized, double-blind, controlled trials • 9 studies involving use of antidepressants for alcohol dependence and MDD met criteria for inclusion • 5 had ns ≤ 20
Reviewing the EvidenceTorrens, Fonseca, Mateu, & Farre (2005) • Improvement in depression • 4 studies SSRIs (Overall OR = 1.85, 95% CI: 0.73-4.68) • 3 other antidepressants (Overall OR = 4.15, 95% CI: 1.35-12.75) • Reductions in drinking • 3 studies SSRIs (Overall OR = 0.93, 95% CI: 0.45-1.91) • 3 other antidepressants (Overall OR = 1.99, 95% CI: 0.78 – 5.08)
Reviewing the EvidenceNunes & Levin (2004) • Double-blind, RCTs with antidepressant vs. placebo groups - 8 involved AUDs • Pooled effect size for HDS scores was 0.38 • Rates of depression response: • 52.1% for the antidepressant group • 38.1% for the placebo group • Examined several potential moderators of treatment outcome including: placebo response, abstinence prior to treatment, gender, psychosocial intervention, type of antidepressant
Reviewing the EvidenceNunes & Levin (2004) • Conclusions: “Antidepressant medication exerted a modest beneficial effect for patients with combined depressive and substance use disorders” • Concurrent therapy targeting addiction is also indicated
Appraising the Evidence • All studies used substance dependence as the criteria for entry – what does this tell us about our patient? • Very small sample sizes in many of the studies (e.g., n’s = 10 and 5 for the antidepressant and control groups, respectively) • Differences in concurrent psychosocial interventions across groups (e.g., CBT vs. “encouraged AA” vs. inpatient) with lower effect sizes and higher placebo response in studies with manual guided interventions
Which Concurrent Therapies are Best? • No studies of comparative effects of different psychotherapies for comorbid depression and AUDs • Integrated interventions have demonstrated some efficacy for other psychiatric and SUD comorbidities – although evidence is limited • Using feasibility as a guide • Largest study of psychosocial treatments for AUDs (project MATCH), brief MET as helpful as more intensive treatments
Motivational InterviewingBurke, Arkowitz, and Menchola (2003) • Review of 30 MI clinical trails – 16 for alcohol use • MI is superior when compared to no-treatment or placebo control and equivalent to other active treatments • Average effect size across studies: • 0.25 – frequency of consumption • 0.53 – blood alcohol concentration • Clinical impact – Reduced drinking by 56% from 36 to 16 standard drinks per week • Clinical utility – prototypical study used 99 minutes of MI • Can be used as a prelude to treatment • Briefer treatment can be combined with antidepressant and has been shown to be as effective as longer treatments
What’s Missing? • Little research on alcohol abuse in the context of depression • Research focus tends to be on primary AUD with secondary depression • Several key questions remain: • Is any drinking okay for patients with MDD? • How does any drinking impact pharmacological treatments? • Psychotherapy outcome? • Consistent with EBM approach, need to integrate research findings with clinical expertise