Download
1 / 49
500 likes | 870 Views
The Etiology of Alcohol Use Disorders. Kenneth J. Sher, Ph.D. Emily Grekin, Ph.D. University of Missouri-Columbia and the Midwest Alcoholism Research Center. Support of authors. Research NIAAA (NIH) Professional Consulting/Reviewing NIH

E N D
The Etiology of Alcohol Use Disorders Kenneth J. Sher, Ph.D. Emily Grekin, Ph.D. University of Missouri-Columbia and the Midwest Alcoholism Research Center
Support of authors • Research • NIAAA (NIH) • Professional Consulting/Reviewing • NIH • Approximately one dozen academic institutions and research centers • Alcoholic Beverage Medical Research Foundation • Joint Defense Group (alcohol industry sponsored legal defense) • Investments • No individual equity position in biotech or health-care related companies (either public or private) • Mutual funds may, and often do, have positions in biotech and health care stocks
Topics to Be Reviewed • Definitions of alcohol-related constructs • Epidemiology of alcohol use, problems, and dependence • Importance of life course and developmental perspectives • Presumed etiological mechanisms • Individual differences in susceptibility • Environmental factors • Towards an integrated perspective
Definitions of Alcohol-related Constructs • Consumption-based measures • Frequency, quantity, and Q-F • Frequency of heavy drinking • Problematic alcohol involvement • Alcohol-related consequences • Alcohol dependence syndrome • DSM-IV alcohol use disorders • Alcohol dependence • Alcohol abuse
DSM-IV Dependence Criteria • Tolerance • Withdrawal • Using in larger amounts/over a longer time period than intended • Persistent desire to cut down/control • Great deal of time spent obtaining/using/recovering • Important activities given up/reduced • Continued drinking despite physical/psychological problems that are caused/exacerbated by alcohol
DSM-IV Abuse Criteria • Failure to fulfill major role obligations • Recurrent use in physically hazardous situations • Recurrent alcohol-related legal problems • Continued drinking despite social/interpersonal problems that are caused/exacerbated by alcohol • Criteria for alcohol dependence not met
Problems with the AUD Definitions • Polythetic criteria • Diagnostic orphans • Diagnostic imposters • Continuum or categories
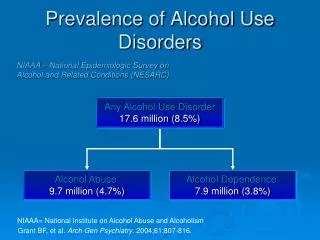
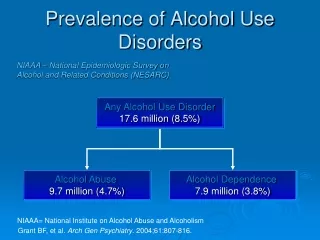
Alcohol Use and AUDs in the Population • Importance of epidemiologic data • Framing the problem • Providing etiological clues • Data from NESARC (2002) • Prevalence of use • Prevalence of heavy drinking • Prevalence of AUDs
Epidemiology of Heavy Use Heavy Use Women: > 1 drink / day Men: > 2 drinks / day Percent
Epidemiological Context • Alcohol use rapidly increases during adolescence, peaking in the early-mid 20s • AUDs show roughly a similar pattern • Implications • Etiological theory needs to address the developmental processes that can help explain this strong, age-graded phenomenon • Processes responsible for desistence (offset) are important for understanding the population prevalence and persistence
Meta-models of AUD Etiology • Pharmacological Vulnerability • Affect Regulation • Negative affect regulation (“self-medication”) • Positive affect regulation (“reward seeking”) • Deviance/Disinhibition
Meta-models of AUD Etiology • Pharmacological Vulnerability • Affect Regulation • Negative affect regulation (“self-medication”) • Positive affect regulation (“reward seeking”) • Deviance/Disinhibition
Pharmacological Vulnerability • Premise: Individual differences in alcohol effects are related to risk for developing AUDs • Insensitivity/tolerance to punishing effects • Insensitivity/tolerance to reinforcing effects • Sensitivity to reinforcing effects • Sensitivity to disinhibition
Pharmacological Vulnerability: Insensitivity to Punishing Effects • Alcohol-related flushing and its relation to drinking rates and AUDs • ADH polymorphisms • ALDH polymorphisms • Other forms of alcohol-related punishment • Headaches and other symptoms? • Hangover?
Pharmacological Vulnerability: Insensitivity to Reinforcement • Low sensitivity and risk for alcoholism • Laboratory findings • Prospective findings • Question of type of effect • Reinforcement or punishment? • Question of BAC Limb • Findings generalized or specific to descending limb?
Pharmacological Vulnerability: Sensitivity to Reinforcement • Positive Reinforcement • Increased arousal • Negative Reinforcement • Stress response dampening • Other measures of effect of alcohol on mood and emotion
Pharmacological Vulnerability: Sensitivity to Disinhibition • Alcohol impairs inhibitory responses • On motor tasks (e.g., go/no-go) • On provoked aggression tasks (e.g., TAP, point subtraction task) • Possible mechanism: disruption of executive functioning • Baseline executive functioning may moderate alcohol/aggression relationship
Meta-models of AUD Etiology • Pharmacological Vulnerability • Affect Regulation • Negative affect regulation (“self-medication”) • Positive affect regulation (“reward seeking”) • Deviance/Disinhibition
Affect Regulation:Negative Mood Regulation • Premise: Alcohol relieves negative moods • Evidence for: • Anxiolytic effects of ethanol in some lab models • “Coping motives” and “tension reduction” expectancies and their relation to drinking • Studies of “stress induced drinking” • Diary studies of drinking and stress/emotions • High comorbidity between anxiety and mood disorders and AUDs • Correlation between negative affectivity/neuroticism and drinking problems
Affect Regulation:Negative Mood Regulation • Evidence against: • Weak correlation between Q-F measures and mood states • Not all lab preparations demonstrate antidepressant or anxiolytic effects • Complexities: • Dose dependency • Effects of chronic alcohol consumption on affective tone…allostasis • Range of emotion-regulation strategies available
Affect Regulation:Negative Mood Regulation • Alcohol can help regulate negative moods and emotions but • Not for all people • Not at all doses • Not in all situations • Protracted heavy consumption may lead to mood dysregulation…regardless of original motivation
Affect Regulation:Positive Mood Regulation • Premise: Alcohol increases positive moods • Evidence for: • Low-moderate doses increase reports of stimulation and euphoria…at least early in the course of intoxication • “Enhancement” motives and generalized expectancies for alcohol as a positively transforming substance are commonly endorsed & correlate with both consumption and problems • Reward seeking (e.g., novelty seeking) is a strong correlate of alcohol consumption
Premise: Alcohol increases positive moods • Complexities: • Alcohol effects seem to be somewhat context dependent (e.g., effects are dose- dependent, person-dependent, subject to tolerance, etc.) • Descending limb effects are typically not positively reinforcing
Meta-models of AUD Etiology • Pharmacological Vulnerability • Affect Regulation • Negative affect regulation (“self-medication”) • Positive affect regulation (“reward seeking”) • Deviance/Disinhibition
Deviance/Disinhibition • Premise: Pathological alcohol use is just a facet of a larger syndrome of externalizing behavior • Evidence for: • Abundance of psychometric work showing that alcohol involvement is associated with a wide range of other “problem behaviors” • Personality traits associated with disinhibition a strong correlate of AUDs • Behavior-genetic studies show a strong genetic correlation between AUDs and other forms of externalizing behavior
Deviance/Disinhibition • Evidence against • No real evidence against but not all individuals suffering from AUDs have an “externalizing” symptom picture…clearly doesn’t explain all cases of AUDs • Complexities • Externalizing behavior can be a determinant as well as a consequence of alcohol involvement • Acutely • Chronically
Etiological Processes • Multiple etiological processes likely operating • Pharmacological vulnerability • Affect regulation • Deviance proneness/Disinhibition • These processes are likely overlapping • Suggest multiple opportunities for prevention and treatment
Risk at the Individual Level • Individual difference variables bias individuals towards different etiological processes • Family history • Personality • Comorbid psychopathology • Alcohol expectancies and drinking motives
Risk at the Individual Level: Family History of Alcoholism • Family history of alcoholism represents one of the best established risk factors for alcohol dependence • Genetic epidemiological studies indicate a substantial role of heredity • Several specific genes appear to convey risk for alcohol dependence
Risk at the Individual Level: Personality • Two broad personality traits appear to be related to risk for AUDs • Traits related to disinhibition/behavioral undercontrol • Traits related to neuroticism/negative emotionality • Traits demonstrated to be important prospectively and to mediate some degree of genetic risk
Risk at the Individual Level: Comorbid Psychopathology • A wide range of childhood and adult disorders associated with risk for alcohol dependence • Childhood and adolescent disorders • ADHD • Conduct Disorder • Mood Disorders
Risk at the Individual Level: Comorbid Psychopathology • Adult disorders • Anxiety Disorders • Depression • Bipolar Disorder • Substance Use Disorders • The special case of tobacco dependence
Comorbid Disorders in Individuals with DSM-III-R Alcohol Dependence Kessler et al, 1997
Risk at the Individual Level: Drinking Motivation • Drinking motives and alcohol outcome expectancies are potent predictors of alcohol involvement • Alcohol outcome expectancies • Beliefs individuals hold concerning the expected outcomes of drinking • Drinking motives • Reasons individuals give for drinking
Risk at the Individual Level: Drinking Motivation • Domains of alcohol outcome expectancies
Risk at the Individual Level: Drinking Motivation • Domains of drinking motives
Risk at the Individual Level: Drinking Motivation • These motivational constructs differentially relate to drinking outcomes in complex ways • “Enhancement” motives • Associated with externalizing traits and predicts problem drinking only through consumption • “Coping” motives • Associated with negative affectivity and predicts problem drinking above and beyond its association with consumption
Risk at the Individual Level: Drinking Motivation • These types of constructs may provide important mediational links between dispositional variables and actual drinking behavior • Expectancies change dynamically, even prior to drinking, and may represent an important modifiable risk factor
Risk at the Environmental Level • Prenatal exposures • Rearing environment/Parenting • Modeling of use • Monitoring • Nurturance/warmth • Abuse and neglect • Peer environment • Life events • Alcohol advertising • Policy surrounding sales and intoxicated behavior • Culture
Risk at the Environmental Level: Some Conceptual Issues • Environment is a multifaceted domain • Biological environment • Interpersonal environment • Policy environment • Cultural environment • Individuals seek out and create their own environments • E.g., Greek organizations on college campuses
Risk at the Environmental Level: Some Conceptual Issues • Person X Environment Interactionism • G x E • More general cases of interactions with environment • Distal Environment vs. Proximal Environment • Effects on traits • Effects on behavioral expression
Towards an Integrated Etiological Perspective • Etiological analyses can be conducted at multiple levels of analysis • Etiological pathways can be conceptualized that link molecular processes (e.g., receptor sensitivity, gene expression) to alcohol seeking but… • Numerous instigating and inhibitory processes need to be considered
Towards an Integrated Etiological Perspective (cont’d) • Etiological mechanisms can be organizing principles for understanding the function of specific risk factors • Etiological heterogeneity • Wide ranging correlates • Heterogeneity in syndrome and course? • Multiple opportunities for prevention and treatment