Download
1 / 28
440 likes | 1.33k Views
Aldosteronism. Armed Forces Academy of Medical Sciences. Outline. Review normal physiology of RAAS system Review normal physiology of Aldosterone Primary hyperaldosteronism Types Symptoms Diagnosis Treatment. Normal Structure of Nephron. Renin-Angiotensin-Aldosterone System (RAAS).

E N D
Aldosteronism Armed Forces Academy of Medical Sciences
Outline • Review normal physiology of RAAS system • Review normal physiology of Aldosterone • Primary hyperaldosteronism • Types • Symptoms • Diagnosis • Treatment
Renin-Angiotensin-Aldosterone System (RAAS) • Controls water reabsorption through the manipulation of sodium reabsorption • Renin release by kidney in response to • Fluid loss • Hypotension • Low Sodium intake • Systemic Vasoconstriction • These factors are sensed by • Baroreceptors (stretch receptors) • Afferent arteriole • Cardiac and arterial baroreceptors • Macula Densa • Early Distal Convoluted Tubule
RAAS Physiology Stimulus Angiotensinogen Arterial Constriction Renin Angiotensin II Angiotensin I Sodium Retention Angiotensin Converting Enzyme (ACE)
RAAS Physiology • Effects of Angiotensin II • Increases Na Retention • Through direct stimulation of the Proximal Convoluted Tubule (PCT) • Increases Aldosterone secretion • Aldosterone increases sodium retention in corticol collecting tubule • Increased Na retention leads to increased water reabsorption • Direct systemic arterial vasoconstriction • Increased blood pressure
RAAS Physiology www.uptodate.com
Aldosterone Synthesis • Synthesized in adrenal cortex • Zona glomerulosa
Normal Mechanism of Aldosterone Action • Increase number of open sodium channels in the luminal membrane of the principal cells in the cortical collecting tubule • Increased sodium reabsorption • Removal of Na makes lumen electronegative • Potassium is secreted from the cells into the electronegative urine to even out charge
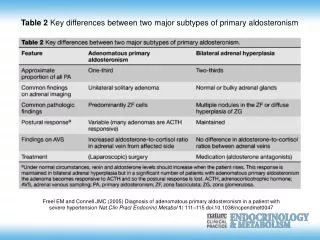
Primary Aldosteronism • Conn’s syndrome • Aldosterone-producing adenoma (30-60%) • Bilateral idiopathic Hyperaldosteronism • Unilateral adrenal hyperplasia • Bilateral macronodular adrenal hyperplasia • Familial hyperaldosteronism • Type 1 • Type 2 • Pure aldosterone-producing adrenocortical carcinomas • Ectopic aldosterone-secreting tumors
Clinical Features of Primary Aldosteronism • Hypertension • Hypokalemia • Metabolic Alkalosis • Other electrolyte abnormalities • Lack of edema
Clinical Features of Primary Aldosteronism: Hypertension • Frequently substantially elevated (> 160 / 100) • Generally resistant to multiple antihypertensive medications • Hypervolemia • Markedly reduces renin secretion • Persistent hypervolemia leads to increased systemic vascular resistance (SVR) • Aldosterone is potent hypertensive agent • Even high normal levels of aldosterone associated with hypertension
Clinical Features of Primary Aldosteronism: Hypokalemia • Increased urinary potassium wasting • Serum potassium remains stable for the short term • Aldosterone induced potassium wasting counterbalanced by potassium retaining effect of hypokalemia • Progressive hypokalemia only occurs if another factor is added • Increased aldosterone production • Initiation of diuretic medication
Clinical Features of Primary Aldosteronism: Hypokalemia • Patients with primary aldosteronism due to adrenal hyperplasia often do NOT have hypokalemia • Phenomenon not understood • Symptoms of hypokalemia • Mild cases are asymptomatic • Mild elevation of blood pressure • Muscle weakness, cramps, myalgias • ECG changes
Clinical Features of Primary Aldosteronism: Other Effects • Metabolic Alkalosis • Due to increased urinary hydrogen ion excretion as a result of aldosterone stimulating Na-H transporter • Mild Hypernatremia • Often between 143 – 147 mEq/L • Hypomagnesemia • Urinary magnesium wasting • Not well understood
Hyperaldosteronism and Cardiac Risk • Patients with primary hyperaldosteronism have higher risk of cardiovascular complications then patients with hypertension • Retrospective study of 124 patients with primary aldosteronism to 465 patients with essential hypertension • Two groups matched for age, gender, degree of BP elevation • Higher rates of stroke, myocardial infarction, atrial fibrillation in hyperaldosteronism group Journal American College Cardiology 2005; 45 (8): 1243
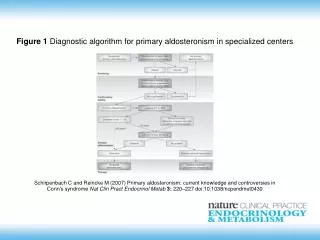
Diagnosis of Primary Hyperaldosteronism • First step is to measure Plasma Renin Activity (PRA) and Plasma Renin Concentration (PRC) • PRA and PRC levels affected by diuretic use • PRA and PRC should be LOW in primary aldosteronism • Measure the Plasma Aldosterone Concentration • Calculate PAC/PRA ratio
Calculating the PAC/PRA ratio • Measure levels at 0800 • Test can be done while patient takes most of his antihypertensive medications • Must hold spironolactone or eplerenone • Will falsely elevated PRA • ACE inhibitor and ARBs will also affect PRA • Normal value of PAC/PRA 4-10 • Primary aldosteronism average 30-50
Interpreting the PAC/PRA ratio • Primary Aldosteronism: PRA suppressed, PAC increased (usually > 15 ng/dL) • PAC > 20 and PAC/PRA > 30 is 90% specific for primary aldosteronism • Secondary Aldosteronism(renovascular disease): PRA and PAC increased, PAC/PRA < 10 • Other (hypercoritsolism, licorice root ingestion): both PRA and PAC suppressed
Establishing Subtype • Adrenal CT • Differentiates adenoma from hyperplasia • Normal adrenal glands does not exclude hyperplasia • Adrenal carcinoma suspected with > 4 cm adrenal mass
Confirming Diagnosis • Adrenal vein sampling • Interventional radiologist obtains aldosterone levels from each adrenal vein • Differentiates bilateral from unilateral disease • Indications for adrenal vein sampling • Confirm unilateral disease in anyone considering surgery • When PAC/PRA is abnormal but CT scan normal
Treatment of Primary Hyperaldosteronism • Treatment or primary aldosteronism is based on whether aldosteronehypersecretion is • Unilateral • Bilateral • Goal of therapy is to prevent morbidity and mortality associated with • Hypertension • Hypokalemia • Increased cardiovascular risk
Treatment of Unilateral Adenoma or Hyperplasia • Surgery: Unilateral adrenalectomy • Unilateral adenoma • Unilateral hyperplasia • Partial adrenalectomy inadequate • Laparoscopic better than open • Shorter hospital stay • Less complications 2008 Endocrine Society Guidelines
Post-Op Management of Unilateral Adrenalectomy • Hypertension and hypokalemia controlled medically • Spironolactone or Eplerenone • Plasma aldosterone should be measured the day after surgery to asses for cure • Patients monitored for hyperkalemia as spironolactone, potassium supplements and anti-hypertensives are discontinued
Medical Therapy for Unilateral Adrenal Hyperplasia or Adenoma • Surgical treatment is preferred method • Medical therapy with aldosterone antagonists is effective • 50 point reduction in systolic BP • 30 point reduction in diastolic BP • Increase in serum potassium of > 1.0 mEq/L • Also include low salt diet, regular exercise • No efficacy difference between spironolactone and eplerenone
Precautions with Spironolactone • Monitor serum potassium and creatinine frequently during first 6 weeks of therapy • Spironolactone will increase half life of digoxin • Concurrent NSAID use will blunt anti-hypertensive effects of aldactone • Patients may develop breast tenderness, decreased libido, gynecomastia
Treatment of Bilateral Adrenal Hyperplasia • Generally milder disease than adrenal adenoma • Less aldosterone secretion • Less severe hypertension and hypokalemia • Patients should be treated with long term aldosterone antagonist • Aldosterone or Eplerenone • May need thiazide diuretic or ACE inhibitor • Partial Adrenalectomy has been tried and failed
Conclusions • Primary hyperaldosteronism is one of the more common causes of hypertension • It often presents as hypertension and hypokalemia • It causes increased cardiovascular morbidity and mortality beyond it’s hypertension • There are many subtypes • Must diagnosis each subtype as treatment varies