Download
1 / 107
1.37k likes | 2.17k Views
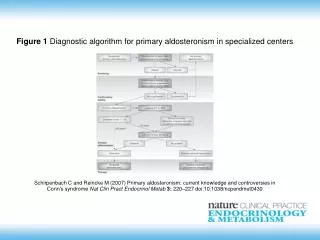
DIAGNOSTIC WORKUP OF PRIMARY ALDOSTERONISM. E ndocrine H ypertension R esearch C entre. Michael Stowasser. Endocrine Hypertension Research Centre, University of Queensland School of Medicine, Greenslopes and Princess Alexandra Hospitals, Brisbane, Australia.

E N D
DIAGNOSTIC WORKUP OF PRIMARY ALDOSTERONISM Endocrine Hypertension Research Centre Michael Stowasser Endocrine Hypertension Research Centre, University of Queensland School of Medicine, Greenslopes and Princess Alexandra Hospitals, Brisbane, Australia UNIVERSITY OFQUEENSLAND
PRIMARY ALDOSTERONISM EXCESSIVE, AUTONOMOUS production of ALDOSTERONE Potassium excretion Salt retention HYPERTENSION SUPPRESSION OF RENIN LOW PLASMA K+ (Hypokalemia)
Harrison's Principles of Internal Medicine, 1991 "…primary aldosteronism accounts for less than 1% of all patients with hypertension…" Clinical Hypertension, 1994 "…the search for primary aldosteronism need only be undertaken in those with hypokalemia…"
Hypokalemic Normokalemic PRIMARY ALDOSTERONISM - Greenslopes (1970-) and Princess Alexandra (2000-) Hospitals Patients Diagnosed Per Year From 1991 - all HTives screened (aldo/renin) Total number of patients with PAL = >1500 Total number undergoing ADX for unilateral PAL = >380 Gordon RD, et al. Lancet 1992 Stowasser M, et al. Mol Cell Endcrinol 2004
PRIMARY ALDOSTERONISM - GREENSLOPES HOSPITAL Out of 199 normokalemic patients referred to the HT Unit without the diagnosis of PAL in mind: - 19 had PAL (9.5%) Gordon RD, et al. Clin Exp Pharm Physiol 1994 Out of 52 patients with HT who volunteered for antihypertensive drug trials: - 6 had PAL (12%) Gordon RD, et al. Clin Exp Pharm Physiol 1993
PREVALENCE OF PAL - SINCE 1997 Some units reporting increased prevalence: Fardella, et al Gong, et al Widimsky, et al Douma, et al Benchetrit, et al Rossi, et al Mulatero, et al Nishikawa, et al (Chile) (China) (Czech Rep) (Greece) (Israel) (Italy) (Italy) (Japan) Eide, et al Loh, et al Rayner, et al MacDonald, et al Young Jr, et al Gallay, et al Calhoun, et al Schwartz, et al (Norway) (Singapore) (Sth Africa) (UK) (USA) (USA) (USA) (USA) Prevalence rates: mostly 5 - 15% Proportion normokalemic: 59 - 100%
Hypokalemic Normokalemic ALDO-PRODUCING TUMORS REMOVED PER YEAR Greenslopes Hospital From 1991 - all HTives screened (aldo/renin) fourfold increase in removal rate cure of HT in 60%; improvement in 100%
John W. Funder, Robert M. Carey, Carlos Fardella, Celso E. Gomez-Sanchez, Franco Mantero, Michael Stowasser, William F. Young Jr, and Victor M. Montori J Clin Endocrinol Metab Sept 2008; 93: 3266-81
SCREENING FOR PAL: ALDO/RENIN RATIO FALSE POSITIVES FALSE NEGATIVES Due to suppression of renin +/- stimulation of aldo Due to stimulation of renin (except hypoK+ - lowering of aldo) Diuretics CCBs (esp DHPs) ACEIs, ARBs V. low salt intake Renovascular HT Malignant HT Hypokalemia Beta blockers a-methyldopa, clonidine NSAIDs Renal impairment Ageing
SCREENING FOR PAL: ALDO/RENIN RATIO FALSE POSITIVES FALSE NEGATIVES Due to suppression of renin +/- stimulation of aldo Due to stimulation of renin (except hypoK+ - lowering of aldo) Diuretics CCBs (esp DHPs) ACEIs, ARBs V. low salt intake Renovascular HT Malignant HT Hypokalemia Beta blockers a-methyldopa, clonidine NSAIDs Renal impairment Ageing
SCREENING FOR PAL: ALDO/RENIN RATIO Correct hypokalemia Unrestricted dietary salt intake Cease diuretics (including spiro) for > 4 weeks Cease beta blockers, a-methyldopa, clonidine, NSAIDs, dihydropyridine CCBs, ACEIs and ARBs for > 2 weeks Substitute with other medications that have a lesser effect on the ratio to maintain HT control - e.g. verapamil slow-release, hydralazine, prazosin Samples collected morning after > 2hours out of bed Patients seated
RECENT STUDIES ON EFFECTS OF OTHER FACTORS ON THE ALDO/RENIN RATIO Gender and hormone changes during the menstrual cycle Contraceptive agents Antidepressants Renin assay method – PRA vs DRC
PRA versus DRC A-II PRA:involves measurement of angiotensin I generated in plasma from the endogenous substrate angiotensinogen by the action of endogenous enzyme renin A-I (The product) Renin (The enzyme) Angiotensinogen DRC:direct measurement of active renin
Could hormonal changes during the menstrual cycle affect the ARR?
How might E2 affect ARR? A-II - Oestrogen stimulates plasma angiotensinogen (renin substrate) production by the liver A-I Renin Renin Angiotensinogen The resultant rise in angiotensin II levels chronically inhibits renal renin secretion by a negative feedback mechanism + Oestrogen
How might progesterone affect ARR? Aldosterone Progesterone antagonizes aldosterone action in the kidney (MR antagonist) - natriuretic effect which in turn stimulates renin and aldosterone secretion Braley et al., 1996 Na+ reabsorption Renin/AngII Distal nephron Na+ excretion Progesterone
Study Design: • Effects of phase of the menstrual cycle on the aldosterone/renin ratio in 21 healthy normotensive female subjects • Influence of renin assay method: direct active renin concentration (DRC) vs plasma renin activity (PRA) • Comparison with 22 healthy normotensive males Ahmed A, et al JCEM 2010
EFFECTS OF PHASE OF MENSTRUAL CYCLE ON THE ARR Pituitary and Ovarian Hormones Values presented as medians (range) Ahmed A, et al JCEM 2010
EFFECTS OF PHASE OF MENSTRUAL CYCLE ON THE ARR Renin, Aldo and ARR Values presented as medians (range) Ahmed A, et al JCEM 2010
EFFECTS OF PHASE OF MENSTRUAL CYCLE ON THE ARR ARR Aldosterone/DRC (pmol/L)/(mU/L) ARR Aldosterone/PRA (pmol/L)/(ng/ml/hr) +P<0.001 Error bars indicate interquartile ranges Ahmed A, et al JCEM 2010
With outliers excluded ARR Aldosterone/DRC (pmol/L)/(mU/L) ARR Aldosterone/PRA (pmol/L)/(ng/ml/hr) +P=0.001 Error bars indicate interquartile ranges Ahmed A, et al JCEM 2010
EFFECTS OF PHASE OF MENSTRUAL CYCLE ON THE ARR ARR in women (according to menstrual phase) versus men *P<0.05 vs Men Values presented as medians (range) Ahmed A, et al JCEM 2010
Discussion • Plasma renin and aldosterone levels are increased in the luteal phase • This is probably due to the markedly increased progesterone secretion. Because progesterone acts as an MR antagonist, it increases natriuresis leading to a rise in renin and aldo production • But why was the change in ARR from follicular to luteal phases greater, and only significant, when DRC but not PRA was used to calculate the ratio?
Possible explanations • A luteal phase increase in angiotensinogen (e.g. estrogen) • Greater generation, in the luteal phase, of angiotensin I (PRA) through enzymes other than renin • Progesterone has been shown to increase the rate of synthesis of cathepsin D A-II A - ACE B A-I Renin B Angiotensinogen A
EFFECTS OF PHASE OF MENSTRUAL CYCLE ON THE ARR Conclusions • When screening women for PAL by ARR, avoiding the luteal phase should minimise the possibility of false positives, and possibly the time of the menses might be optimal when estrogen and progesterone levels are at their lowest and the ARR range is closest to male • Should we consider different reference ranges for men and women? Ahmed A, et al JCEM 2010
CONTRACEPTIVES AND THE ARR • Because both estrogen and progesterone affect aldo and renin levels, we studied effects of two contraceptives commonly used in our population, one oral and one subdermal, on ARR • Methods: • normotensive, healthy women (family planning clinic) • upright plasma aldo, DRC, PRA measured • baseline (menses) and after either: • 3 weeks oral ethinylestradiol plus drospirenone (EE+D, “Yaz”; n=17) or • 1 and 6 weeks sub-dermal etonogestrel (ETO, “Implanon”; n=15), a third generation progestin Ahmed A, et al JCEM 2011
Effects of Oral EE+D (Yaz) Ahmed A, et al JCEM 2011
Effects of Oral EE+D (Yaz) ARR with DRC DRC ARR with PRA PRA Aldo Cortisol
Effects of Subdermal ETO (Implanon) Ahmed A, et al JCEM 2011
Effects of Subdermal ETO (Implanon) ARR with DRC DRC ARR with PRA PRA Aldo Cortisol
CONTRACEPTIVES AND THE ARR • Results: • Treatment with EE+D was associated with significant increases in aldo and PRA but decreases in DRC, leading to increases in ARR calculated by DRC but not by PRA • In contrast, treatment with subdermal ETO was associated with no significant changes in PRA, DRC, aldosterone or ARR at either one week or six weeks • Conclusion: • The combined oral contraceptive ethinylestradiol plus drospirenone is capable of significantly increasing ARR with risk of false positive results during screening for PA, but only if DRC is used to calculate the ratio Ahmed A, et al JCEM 2011
Yaz • estrogen stimulates angiotensinogen production by the liver • resultant rise in ang II levels chronically inhibits renal renin secretion by negative feedback • hence peripheral blood DRC falls (so the ARR calculated by DRC increases) • drospirenone has anti-mineralocorticoid activity by competing with aldo at the mineralocorticoid receptor • consequently, PRA, angiotensin II and aldo increase • hence, the ARR calculated using PRA does not change significantly probably because both aldo and PRA rise • rise in cortisol after commencing Yaz may be due to increased production of cortisol binding globulin by estrogen • Implanon • implantable progestin-only contraceptive which releases etonogestrel (active metabolite of desogestrel, a progestin derived from testosterone) • it is possible that progestins of this type, unlike progesterone and drospirenone, have no appreciable effect on components of RAAS • lack of estrogen in this preparation may explain the lack of effect on DRC • subdermal implantation is associated with less effects on the liver
ANTIDEPRESSANTS AND THE ARR • There are no previously published data on the effects of antidepressants on ARR • Methods: • normotensive, depressed male patients (n=26) • upright plasma aldo, DRC, PRA • baseline, and after 2 and 6 weeks treatment with • sertraline (n=14) or • escitalopram (n=12) Both SSRI antidepressants
Effects of Sertraline ARR with DRC DRC PRA ARR with PRA Aldo Cortisol
Effects of Escitalopram ARR with DRC DRC PRA ARR with PRA Aldo Cortisol
How might SSRIs affect the ARR? • serotonin may stimulate renin via the 5-HT2 subtype of 5-HT receptors • serotonin has been reported to increase aldosterone levels • chronic administration of SSRIs has been reported to decrease ACTH, which may explain why cortisol levels fell • acutely, a fall in ACTH may also have influenced aldo levels and may or may not explain the lesser increase in aldo compared to renin, and hence the fall in ARR • chronic administration of SSRIs has been reported to cause inhibition of the SNS, so this is unlikely to explain the rise in renin
ANTIDEPRESSANTS AND THE ARR • Results: • For both SSRI antidepressants, treatment was associated with rises in aldo, DRC and PRA • ARR fell significantly whether calculated using DRC or PRA • Conclusions: • SSRI antidepressants can significantly reduce ARR and therefore potentially increase the risk of false negative results when screening for PA • Further studies in hypertensive patients, including patients with confirmed PA, are required
SUMMARY • The ARR is higher in women than men • The ARR is higher in the luteal phase than during menses or the follicular phases and can be falsely positive during the luteal phase, but only when measured by DRC and not by PRA • The ARR rises and is associated with false positive values when using DRC (but not PRA) during treatment with the combined oral contraceptive Yaz, containing ethinyl estradiol and drospirenone • SSRI antidepressants are associated with a fall in the ARR, and hence may raise the risk of false negative ratios in patients with PA
SCREENING FOR PAL: ALDO/RENIN RATIO FALSE POSITIVES FALSE NEGATIVES Diuretics CCBs (esp DHPs) ACEIs, ARBs V. low salt intake Renovascular HT Malignant HT Hypokalemia SSRI antidepressants Beta blockers a-methyldopa, clonidine NSAIDs Renal impairment Ageing Females – luteal phase Some OCPs – Yaz (A Ahmed, et al JCEM 2010 and 2011)
ALDO/RENIN RATIO: CUT-OFF VALUES = 20 Aldo in ng/dL; PRA in ng/mL/h = 200 Aldo in pg/mL; PRA in ng/mL/h = 550 Aldo in pmol/L; PRA in ng/mL/h = 70 Aldo in pmol/L; DRC in mU/L Conversion factors Aldo: 1 ng/dL = 27.7 pmol/L Renin: 1 ng/mL/h (PRA) = 8.4 mU/L (Direct Renin)
ALDO/RENIN RATIO: CUT-OFF VALUES = 20 Aldo in ng/dL; PRA in ng/mL/h = 200 Aldo in pg/mL; PRA in ng/mL/h = 550 Aldo in pmol/L; PRA in ng/mL/h = 70 Aldo in pmol/L; DRC in mU/L Conversion factors Aldo: 1 ng/dL = 27.7 pmol/L Renin: 1 ng/mL/h (PRA) = 8.4 mU/L (Direct Renin)
Should we use a cutoff level for plasma aldosterone? e.g. 15 ng/dL (~410 pmol/L)
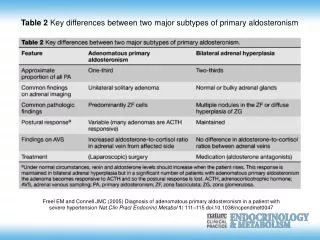
Unilateral (n=21) 6 (29%) 51 ± 2 9 (43%) 7 (33%) 11 (52%) 29 ± 3 0.4 ± 0.1 128 ± 21 4 (19%) 14 (70%) 10 (48%) (9 ipsi, 1 contra) Bilateral (n=42) 20 (48%) 53 ± 1 2 (5%) 17 (41%) 18 (43%) 19 ± 1 0.4 ± 0.1 68 ± 9 18 (43%) 32 (76%) 8 (19%) P-value n.s. n.s. <0.001 n.s. n.s. <0.01 n.s. <0.05 n.s. n.s. <0.05 Female Age (yrs) No. hypokalemic No. with “resistant” HT No. with either Upright plasma aldo (ng/dL) Upright PRA (ng/ml/h) Upright ARR No. with plas aldo <15 ng/dL (<410 pmol/L) No. with aldo posture-resp No. with unilateral CT mass M Stowasser et al. Mol Cell Endocrinol 2004
THE IMPORTANT OF CONFIRMATORY TESTING The aldo/renin ratio is a screening test only – even when confounding factors controlled, false positives can occur – should be repeated at least 1-2 times After definitive diagnosis of PAL, further diagnostic testing to determine the subtype is expensive, and, in the case of adrenal venous sampling (the most reliable means of differentiating unilateral from bilateral forms of PAL), relatively invasive and not without risk (esp. adrenal venous hemorrhage)
CONFIRMATORY TESTING FOR PAL - FLUDROCORTISONE SUPPRESSION TEST Plasma aldo response during 4 days administration of fludrocortisone (0.1 mg 6 hrly) and Slow Na+ (30 mmol tds) with sufficient dietary salt to achieve urinary Na+ excretion rate of at least 3 mmol/kg/day Failure of upright (1000 h) aldo to suppress to <165 pmol/L (<6.0 ng/100mL) by day 4 diagnostic of PAL PROVIDED THAT… 1) 2) Renin suppressed (<8.4 mU/L for DR, or <1 ng/mL/h for PRA) K+ normal (measured 3-4 times daily; sufficient Slow K given 6 hrly to keep plasma K+ close as poss to 4.0 mmol/L) Comparison of plasma cortisol levels at 0700h and 1000h on day 4 does not suggest an acute rise in ACTH 3)
Fludrocortisone suppression test: DAY Basal Day 4* SAMPLE Rec (0700 h) Up (1000 h) Rec (0700 h) Up (1000 h) ALDO (pmol/L) 388 943 239 913 RENIN (mU/L) <2 5.0 <2 2.5 K+ (mmol/L) 3.6 3.6 3.9 4.0 CORTISOL (nmol/L) 512 420 391 314 i.e. PAL CONFIRMED *24h urinary Na+ (collection completed 1000 h Day 4) = 277 mmol (3.8 mmol/kg)
OTHER CONFIRMATORY TESTS FOR PAL Saline infusion test - plasma aldo following i.v. infusion of normal saline (2L over 4h) >140-280 pmol/L (>5-10 ng/100 ml) Urinary aldo after oral salt loading - 24h urinary aldo following 3 days of oral salt loading (>200 mmol sodium/day) >12 ug/d Captopril challenge test - aldo/renin ratio (seated) 60 mins after oral captopril (50 mg) >30
EVALUATION OF SALINE INFUSION TEST (2L over 2h) Saline Infusion Test Positive* n Patients with positive FST 97 17 (18%) Patients subseq cured of PAL by unilateral ADX 10 3 (30%) *Post-saline recumbent plasma aldo >220 pmol/L (>8.0 ng/dL)