Download
1 / 26
420 likes | 1.37k Views
Primary Aldosteronism. Paul S. Kellerman, M.D., FACP Associate Professor Division of Nephrology. 65,000,000, 31% of adults (1999-2000) (Fields et al, Hypertension, October 2004). EPIDEMIOLOGY OF HYPERTENSION. U.S. PREVALENCE 50,000,000, 27% of adults (1988-94)

E N D
Primary Aldosteronism Paul S. Kellerman, M.D., FACP Associate Professor Division of Nephrology
65,000,000, 31% of adults (1999-2000)(Fields et al, Hypertension, October 2004) EPIDEMIOLOGY OF HYPERTENSION U.S. PREVALENCE 50,000,000, 27% of adults (1988-94) WORLDWIDE PREVALENCE 1,000,000,000
FREQUENCY OF VARIOUS DIAGNOSES IN HYPERTENSIVE PATIENTS – 1980s PRIMARY CAREREFERRAL Essential 92-95% 89% Chronic kidney dis 3-6% 5% Renovascular dis 0.2-1.0% 4% Pheochromocytoma 0.1-0.2% 0.2% Aldosteronism 0.1-0.3% 0.5% Cushing’s syndrome 0.1-0.2% 0.2% Coarctation 0.1-0.2% 1% Oral contraceptives 0.2-1.0%
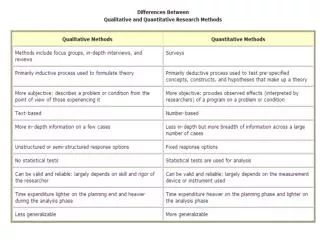
DIFFERENTIATION OF SECONDARY FROM ESSENTIAL HYPERTENSION • Know presentation and course of essential hypertension • Know signs and symptoms of secondary etiologies
Essential Hypertension • Onset in 30s and 40s • Gradual onset • Gradual progression of HTN/slow addition of medications • Lack of severe end-organ damage • Family history • Often associated with obesity • Lack of signs and symptoms of secondary causes • Lack of laboratory evidence of secondary causes
Secondary Hypertension • Hypertension onset at age extremes <30 >50 • Rapid onset of severe hypertension • More severe chronic end-organ damage • Grade III/IV retinopathy, LVH/CHF, CKD • Lack of family history • Sign and symptoms of secondary etiologies • Laboratory evidence of secondary etiologies • Emergent hypertension • Resistant hypertension
Primary Aldosteronism Secondary cause of hypertension due to excessive secretion of aldosterone from the adrenal gland, due either to tumor or hyperplasia.
FREQUENCY OF VARIOUS DIAGNOSES IN HYPERTENSIVE PATIENTS - 2007 PRIMARY CAREREFERRAL Essential 92-95% 89% Chronic kidney dis 3-6% 5% Renovascular dis 0.2-1.0% 4% Pheochromocytoma 0.1-0.2% 0.2% Aldosteronism 5-13% Cushing’s syndrome 0.1-0.2% 0.2% Coarctation 0.1-0.2% 1% Oral contraceptives 0.2-1.0%
When to Screen for Aldosteronism • Hypertension and Spontaneous Hypokalemia • Hypertension and Adrenal Tumor • Resistant Hypertension (20% incidence)
Incidence of Aldosteronism Increases with Hypertension Severity Mosso L et al. Hypertension 42:161, 2003
Laboratory Screening • Plasma aldosterone concentration (PAC) and plasma renin activity (PRA) • Drawn from ambulant seated patient • Morning blood draw • Potassium must be normalized (not hypokalemic) to avoid false suppression of aldosterone
Positive Screening Meriting Further Investigation for PA Aldosterone-Renin Ratio (ARR)>30 (20-60?) – PRA is normalized to 0.5 if <0.5 AND Aldosterone level>15 ng/dL
Potential Alterations in ARR with Medications Do we need to stop medications for ARR? • Beta-blockers • False +ARR (lower renin, but also therefore lower aldosterone) • Angiotensin receptor blockers (>ACE Inh) • False –ARR (lower aldosterone, raises renin) • Diuretics • With thiazides and loop diuretics, may not be much effect, since raise both aldo and renin, so ratio doesn’t change much • Spironolactone should be stopped (increased aldosterone) • Calcium channel blockers • Minimal effects May not matter for ARR(Gallay BJ, et al. Am J Kidney Dis 37:699-705, 2001)
Aldosterone Suppression Tests %ARR with lack of suppression – mean 60% , range26-95% (Kaplan NM, J Hypertension 22:863-69, 2004) • IV Saline suppression • 500 mL 0.9% NaCl/hr for four hours OR 500 mL 0.9% NaCl over 30 minutes, then 500 mL/hr for 2 hours (1.5 liters over 2.5 hours) • Draw PAC at time 0, 120, 150 minutes for short test • Suppression if PAC <8.5 ng/dL (<6 normal >10 PA) • Oral sodium chloride suppression test • 10 gms NaCl daily for 4 days • On day 4, collect 24 hour urine aldosterone, sodium • Suppression if aldosterone<14 mcg and sodium > 200 mEq/24 hours • Fludrocortisone suppression test • high salt diet and large doses of Florinef over a 4 day hospitalization
Imaging for Aldosteronism • CT – thin cuts of adrenal glands • MRI • 131-I-iodocholesterol
Imaging for Aldosteronism • Problems with CT/MRI • Lots of False Positives • Only can image adenoma if > 1cm • Of these, 1/3 are incidentaloma (no lateralization on adrenal vein sampling) • Lots of False Negatives • Up to 1/3 of adenomas are missed because of small size (lateralize on adrenal vein sampling)
Role for Adrenal Vein Sampling When to use: Unilateral adenoma > 40 years old “High risk APA” with normal adrenals on CT scan or mild asymmetry
Role for Adrenal Vein Sampling “High Probability” APA Severe HTN Hypokalemia (<3) Higher Aldo levels plasma >25 ng/dL urine > 30 mcg/24 hrs Age < 50 BUT: AVS is only good in very experienced hands – technically very difficult
Therapy • If tumor with lateralization, laparascopic adrenalectomy • If tumor without lateralization (incidentaloma), or hyperplasia, then aldosterone blockade • Spironolactone • Eplerinone
Primary Aldosteronism in 2007 • The incidence of primary aldosteronism due to adrenal hyperplasia as defined by saline suppression is much higher than previously thought. • Hypokalemia is often not present with hyperplasia and is not a sine qua non for diagnosis. • Resistant hypertensives have a high incidence of primary aldosteronism. • Controversy exists as to definitive ARR thresholds, medication use during suppression testing, and adrenal imaging. • AVS is the “gold standard” but not often available due to technical limitations
Case • Does she have hyperaldosteronism? • Likely, but not confirmed • If so, is this hyperplasia or adenomatous (did the CT miss it)? • Unlikely adenoma, given age, very mild hypokalemia (almost normokalemia), HTN severity • Is the treatment appropriate?
UW HYPERTENSION CLINIC • Multidisciplinary HTN clinic • Nephrology (Kellerman) • Cardiology (Moncher) • Endocrinology (Shenker) • At the UW Kidney Clinic on Fish Hatchery Road • 270-5656