Download
1 / 24
240 likes | 263 Views
Learn about the gross anatomy of the skeletal system, including the membranes and bone development processes. Understand the chemical composition of bone and the different types of ossification. Explore the concepts of interstitial and appositional growth in bone.

E N D
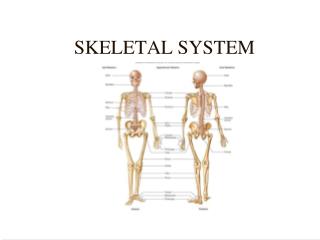
Biology 220 Anatomy & Physiology I Unit XIISKELETAL SYSTEM Take a quiz on bones at: http://occawlonline.pearsoned.com/bookbind/pubbooks/mariebhap/chapter6/multiple2/deluxe-content.html Chapter 6 pp. 172 - 197 E. Gorski/E. Lathrop-Davis/S. Kabrhel
Gross Anatomy - Membranes • Periosteum (peri = around, osteo = bone) • double-layered membrane: • fibrous - outer layer (dense irregular connective) • osteogenic - abuts the bone; contains osteoblasts (“bone germinators”) and osteoclasts (“bone breakers”) • nerve fibers, lymphatic and blood vessels • provides insertion for tendons and ligaments • Endosteum (endo = within) • delicate connective tissue layer • covers trabeculae of spongy bone in marrow cavities; lines medullary cavity; lines the central (Haversian) canal • contains osteoblasts and osteoclasts
Chemical Composition of Bone • Proper combination of organic and inorganic matrix elements gives strength and durability 1. Organic components(~ 35%): • cells: osteblasts, osteoclasts, osteocytes • osteoid (organic component of matrix): consists of proteoglycans, glycoproteins, collagen fibers (all secreted by osteoblasts) 2. Inorganic components (~65%): • hydroxyapatites (mineral salts), largely calcium phosphates
Bone Development (Osteogenesis or Ossification) • The skeleton initially made up of : • hyaline cartilage • elastic cartilage • fibrocartilage • Ossification begins in the second month of gestation • Intramembranous: • within fibrous CT (mesenchyme -->bone) • forms flat bones (most cranial bones and clavicles) • Endochondral: • within hyaline cartilage • mesenchyme --> cartilage --> bone • forms most bones http://www.sru.edu/depts/pt/histo/neonatal.htm
Intramembranous Ossification Steps: 1. Mesenchymal cells at centers of ossification differentiate into osteoblasts 2. Osteoblasts secrete organic bone matrix within membrane: • followed by calcification • trapped osteoblasts mature into osteocytes Fig. 6.7, p. 181
Intramembranous Ossification 3. Blood vessels enter ossified area resulting in formation of spongy bone (red bone marrow inside) 4. Outer layer of bone reorganized into compact bone • remaining fibrous tissue outside ossified tissue becomes periosteum Fig. 6.7, p. 181
Intramembranous Ossification http://education.vetmed.vt.edu/Curriculum/VM8054/Labs/Lab8/Examples/exmembos.htm
Endochondral Bone Formation • Ossification begins at primary ossification center (in cartilage at middle of shaft for long bone); continues at secondary ossification centers • in short bones - only have primary ossification centers • in irregular bones - have several ossification centers
Endochondral Bone Formation Ossification begins at primary ossification center (in cartilage at middle of shaft for long bone) Steps (long bone): 1. Formation of bone collar: • blood vessels enter perichondrium at middle of shaft • selected mesenchymal cells (called osteoprogenetor cells) become osteoblasts • osteoblasts secrete bone matrix creating a bone collar
Endochondral Bone Formation 2. Secretion of organic matrix causes chondrocytes in shaft to hypertrophy (signals calcification) and these cells eventually burst resulting in cavity 3. Formation of periosteal bud blood vessels, nerve fibers, osteoblasts, osteoclasts enter shaft --> form spongy bone
Endochondral Bone Formation 4. Diaphysis elongates as primary ossification center spreads proximally and distally; medullary cavity forms 5. Formation of secondary center(s) of ossification in one (or both) epiphysis around time of birth (like primary but spongy bone remains) • When secondary ossification completed hyaline cartilage remains as: • articular cartilage • epiphyseal plate Fig. 6.8, p. 182
Endochondral Bone Formation http://www.uoguelph.ca/zoology/devobio/210labs/meso2.html
Postnatal Bone Growth: 1. Interstitial Growth (length) • cartilage cells in epiphysial plate form tall columns: • zone 1 - growth zone (dividing chondrocytes) (zone of proliferation) • zone 2 - transformation zone (zone of hypertrophy and calcification), closer to shaft, chondrocytes enlarge then die, matrix calcifies
Postnatal Bone Growth: 1. Interstitial Growth (length) • zone 3 - osteogenic zone (zone of retrogression and ossification), long spicules of calcified cartilage form at the epiphysis-diaphysis junction and become covered with bone matrix of spongy bone (tips later digested by osteoclasts to enlarge medullary cavity) • at adolescence, chondrocytes divide less often epiphysial plate becomes thinner -> entirely replaced by bone between age 18-21 years.
2. Appositional Growth (thickness) • osteoblasts in periosteum secrete bone matrix on external surface of bone • osteoclasts on endosteal surface (diaphysis) remove bone • more built than broken matrix -> bone gets thicker Fig. 6.10, p. 184
Hormonal Regulation of Bone Growth 1. Growth hormone (GH) • active from infancy through childhood • acts on epiphyseal plate to stimulate division of chondrocytes • disorders • gigantism - hypersecretion of GH • dwarfism - hyposecretion of GH or T3/T4 2. Calcitonin - inhibits osteoclast activity 3. Parathyroid hormone - stimulates osteoclast activity
Hormonal Regulation of Bone Growth 4. Thyroid hormones (T3 and T4) modulate activity of cells in response to GH to ensure proper proportions of the skeleton 5. Sex hormones (testosterone and estrogens) • active at puberty • initial growth spurt (hormones stimulate osteoblasts) • masculinization or feminization (affects shape of bone) • later, cause epiphyseal plate to close
Bone Remodeling • 5-7% of bone mass recycled every week (distal femur fully replaced every 5-6 month) • spongy bone replaced every 3-4 years, • compact bone replaced every 10 years • Remodeling occurs at periosteal and endosteal surfaces • Bone deposit - formation of osteoid followed by later mineralization • Bone resorption - osteoclasts secrete lysosomal enzymes that digest the organic matrix and metabolic acids that digest calcium salts (release calcium)
Control of Bone Remodeling • Blood calcium requirement • 400-800 mg/day (child) • 1200-1500 mg/day (young adult) 1. Hormonal control • PTH released when blood calcium level declines • increases osteoclast activity • calcitonin released when blood calcium level rises • inhibits osteoclast activity • promotes osteoblast activity 2. Mechanical stress • heavy usage leads to heavy bones • disuse leads to wasting Fig. 6.11, p.186
Bone Repair Steps (simple fracture): 1. Formation of hematoma - mass of clotted blood forms at the fracture site 2. Formation of fibrocartilaginous callus (soft callus = granulation tissue) • capillaries and phagocytic cells invade hematoma • fibroblasts secrete collagen fibers • osteoblasts begin formation of spongy bone
Bone Repair 3. Formation of bony callus (hard callus) • new bone trabeculae appear in fibrocartilaginous callus and gradually convert into hard bone (callus) 4. Remodeling - excess material in bone shaft exterior and within the medullary cavity is removed and hard wall are remade *Healing time of simple fracture: 6-8 weeks (sometimes as few as 3 weeks) Fig. 6.13, p. 189
Examples of Common Types of Fractures • closed (simple) - completely internal • open (compound) - bone ends penetrate the skin • linear - break parallels the long axis of the bone • transverse - break across the bone long axis • complete - bone is broken through • incomplete (greenstick) - on side of the shaft breaks, the other side bends
Bone - Homeostatic Imbalances 1. Dietary Causes: Insufficient calcium, vitamin D, vitamin C: • Osteomalacia - soft bone, inadequate mineralization, pain when weight is applied • Rickets- soft bones in children, bowed legs, deformities of pelvis, skull, and rib cage
Bone - Homeostatic Imbalances 2. Other Known Causes: Estrogen deficiency, insufficient calcium, protein deficiency, abnormal vitamin D receptors, immobility, hyperthyroidism, diabetes: • Osteoporosis - bone resorption outpaces bone deposit 3. Unknown Cause (probably initiated by virus): • Paget’s disease - excessive bone formation and break down leading to weakened bones, irregular thickening, and/or filling of marrow cavities