Download
1 / 53
540 likes | 783 Views
Glial responses to TBI. Gliosis (change in glial cells) common after injury - esp. astrocytes form glial scar that re-establishes physical and chemical integrity of CNS. Whereas adult neurogenesis is focal/limited, glial responses widespread/robust.

E N D
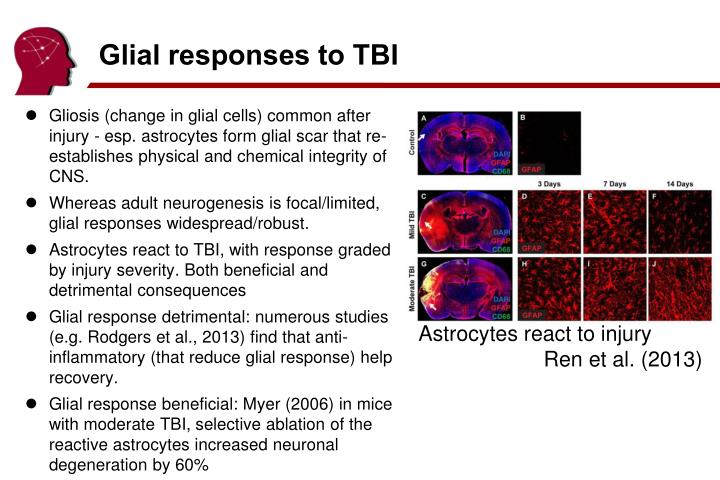
Glial responses to TBI • Gliosis (change in glial cells) common after injury - esp. astrocytes form glial scar that re-establishes physical and chemical integrity of CNS. • Whereas adult neurogenesis is focal/limited, glial responses widespread/robust. • Astrocytes react to TBI, with response graded by injury severity. Both beneficial and detrimental consequences • Glial response detrimental: numerous studies (e.g. Rodgers et al., 2013) find that anti-inflammatory (that reduce glial response) help recovery. • Glial response beneficial: Myer (2006) in mice with moderate TBI, selective ablation of the reactive astrocytes increased neuronal degeneration by 60% Astrocytes react to injury Ren et al. (2013)
Concussions and permanent injury • Some suggest the mildest TBIs cause no permanent injury: • American Association of Neurological Surgeons: “experts emphasize that although some concussions are less serious than others, there is no such thing as a ‘minor concussion’. In most cases, a single concussion should not cause permanent damage” • On the other hand, even if symptoms typically ~7 days, unclear if there is not subtle permanent injury. • If no lasting injury, what is the mechanism for transient cognitive dysfunction? • Can this explain vulnerability for 2nd injury? • Popular models suggest all TBIs cause chemical cascade, this can either resolve or lead to permanent 2nd injury.
Lifestyle: Football and dementia • Savica et al. (2012) no significant difference between high school football (‘46-’56) and band Lehman et al. (2012)3439 NFL players from ‘59-’88. AD/ALS x4 expected, esp. Speed. Vanacore (2013): not necessarily due to TBI: perhaps intense physical activity, use of drugs, exposure to neurotoxins
Biochemical changes in TBI • Concussion (mTBI) lead to behavioral changes that typically resolve ~7 days (discussed last week) • Understanding mechanism is important • Biomarkers for return to play • Are all concussions permanent TBI, or are some simply transient biochemical imbalances? • Might help treatment (prevent 2nd injury)
Neuron Chemistry • Neurons firing via electro-chemical signals. Requires energy gradient to work. • Potassium/Sodium pumps expel two sodium and intake two calcium ions. • Net result, neuron rests at -70mV • 70% of the energy is used to maintain the Na+, K+ membrane potentials. • Pumps work continuously to keep gradients, firing causes rapid, large brief expense of energy. • When cell fires: • sodium channels briefly open: sodium rushes in: neuron briefly has positive voltage (+30mV) • next, potassium channels briefly open, potassium rushes out, voltage restored • Refractory period • Absolute: Neuron can not re-fire while sodium channels open • Relative: Low sensitivity while potassium channels open K+ K+ Na+ Na+ Na+
Cellular Respiration • Fueling neurons (can not use free fatty acids) • Create pyruvate • Anaerobic Glycolysis (Primary) • Convert glucose to pyruvate and 2 ATP • Occurs in Cytoplasm • Ketone bodies (starvation, worst-case) • Use Pyruvate • Aerobic (‘Conversion’, sustained, primary): • Where: Mitochondria • Efficient (36 ATP) • Requires: O2 • Waste: CO2, free radicals (specifically, reactive oxygen species [ROS]) • Anti-oxidant enzymes to counteract free radicals • Anaerobic (‘Fermentation’, burst, backup) • Where: Cytoplasm • Inefficient (2 ATP) • Waste: Lactic Acid (marker for fermentation)
Metabolism • Human Brain about 2% of body weight, 20% of energy. • Brain: glucose is principal fuel, ketone is emergency backup. • Rest of body: glucose or fatty acids. • Humans have relatively large brain/body (high energy demands) with large energy reserves (fat). • Other animals: ~5% energy at rest • When fasting (or extremely low carb diet): • <0.25 days: glycogen reserves • 0.25..3 days: fat converted to free fatty acids and glucose • >3 days: liver converts fatty acids to ketones (@4 days, 70% of brain metabolism is from ketones). Even so, not enough glucose comes from fat breakdown, so additional glucose must come from breakdown of proteins (e.g. muscle). • Other mammals: Fat breakdown typically provides sufficient amount of glucose. No need to produce ketones or break down proteins. • Ketogenic diet controls pediatric epilepsy, potentially because calorie restriction, fewer free radicals, acidic (blocks ion channels), less glucose, more inhibitory GABA.
Understanding 2nd Injury • Barone & Feuerstein (1999) [for ischemic stroke] Necrosis: cell death - contusion and border, hippocampus Apoptosis: cell suicide - not due to membrane failure, glutamate mediated, minimal immune response
Neurometabolic Cascade • Giza & Hovda (2001) Sequence of biochemical changes after TBI. • Initial (minutes) • K+ increase • Glutamate release • Lactate increase • Sustained (days) • Blood flow (CBF) decrease • Ca+ increase • Biphasic • cerebral metabolic rate (CMR) of glucose initially increased, then decreased
Why is glucose usage reduced? • Clear evidence TBI leads to chemical changes • Mechanism debated. Two (not mutually exclusive) options: • Decreased need for glucose metabolism. E.G. Pappius (1995) suggest noradrenergic and serotonergic reductions. • However, these effects appear short lived (hours), whereas CBF disturbed for days. • Metabolic dysfunction, e.g. Giza & Hovda’s neurometabolic cascade
Neurometabolic Cascade • Giza & Hovda (2001) Model to explain sequence of Neurometabolic Cascade. • Initial injury: membranes injured, glutamate and K+ leak into extracellular space. • Ionic pumps work overtime K+, exhausting ATP. • Glutamate causes influx of calcium. • Glucose uptake initially increases, but Calcium overload makes aerobic conversion inefficient. • Claim: mTBI is primarily cellular dysfunction and little cell death, where in more severe TBI calcium leads to apoptosis.
Neurometabolic Cascade • Giza & Hovda (2001); Barkhoudarian, Hovda, Giza. (2011) • Cell membrane deformed/leaky: Glutamate released, Ca+ influx • Glutamate activates post-synaptic NMDA, Releasing K+, Intake Ca+ • Ionic pumps attempt to restore gradient (pump in K+, pump out Na+). This requires ATP • ~30 minutes: Hyperglycosis to create ATP • ATP demands lead to Lactate accumulation and Ca+ influx of mitochondria. • 30min-5days, mitochondria function inefficient: decreased glucose metabolism (50%) decreased aerobic activity, increased free radicals.
Neurometabolic Cascade • Barkhoudarian et al. (2011) • hyperglycolysis and oxidative dysfunction ~30 min post injury. • Anaerobic glycolysis is the transformation of glucose to pyruvate when limited amounts of oxygen (O2) are available • Inefficient anaerobic function designed for short bursts - limited reserves. • ~6hrs post injury: glucose hypometabolism (approximately 50%). Lasts ~5days (mild) ~months (severe) • Tissue vulnerable to subsequent injury during this period • In mild cases cells eventually return to normal function, in severe cases apoptosis.
Human evidence for metabolic cascade • Vespa et al. (2005) Often small primary injury includes widespread dysfunction as observed by decreased oxidative metabolism (CMRO2) and altered glucose metabolism. • Little Post-traumatic ischemia • Ongoing metabolic crisis (elevated lactate/pyruvate ratio, LPR) • Found LPR (anaerobic) negatively correlated with CMRO2 (aerobic)
Human evidence • Stein et al. (2012) evaluated 72 individuals with controlled ICP during initial 72h of severe TBI. • 76% Low glucose • 93% elevated lactate/pyruvate ratio (LPR) >25 • Lactate produced by pyruvate only under anaerobic conditions • 74% metabolic crisis (both low glucose and high LPR) • Metabolic crisis predicted poor 6 month outcome
Cascade Implications • Cascade model suggests glucose conversion transiently disrupted. • Switching to ketones when glucose use is disrupted may be beneficial. • Recent studies suggest ketone neuroprotective (Prins, 2008) and post-injury (Prins et al., 2005; Deng-Bryant et al., 2011) in younger rats. • Perhaps fasting/ketogenic diet useful for mTBI
Cascade Summary • Barkhoudarian et al. (2011) Implications • Return to play: "concussion-induced pathophysiologic conditions, as manifested by metabolic perturbations, altered blood flow, axonal injury, and abnormal neural activation, reduce cerebral performance and make the brain more susceptible to cellular injury” • Appears to suggest that some mTBI may be transient biochemical imbalance rather than permanent injury.
Vulnerable window • Prins et al. (2013) Glucose metabolism altered in rats for ~7 days (differs with age and injury). • 2nd injury in this timeframe will have severe consequences • Why? Perhaps poor auto regulation since CBF and metabolism uncoupled.
Evidence for vulnerable period • Humans: initially vulnerable to 2nd TBI • Is this biochemical or psychological (poor awareness)? • Recent animal studies suggest ~7day window of vulnerability for 2nd injury. • Mice: Longhi et al (2005) • Rats: Vagnozzi et al. (2007) Tavazzi et al. (2007) • This data proves biochemical involvement
Axon disconnection • Park et al. (2008): In addition to damage to gray matter, specific secondary effects influence axonal disconnection • Impaired microcirculation due to stenosis and • astrocyte foot swelling • Proliferation of glial cells • Excess glutamate • Calcium Influx • Excitotoxicity • Ca accumulation • Disconnection
Pause • Break
Predictors of TBI prognosis • Considerations • Severity/Mechanism • Pre-injury function • Age • Health • Gender • Genetics (APoE e4) • Resources • http://mitbitraining.org • http://www.nctbitraining.org/main.aspx
TBI Classification • Mechanism • Closed vs. Open • Open: Penetrating vs. Perforating • Pathology • General: Primary vs. Secondary Injury • Blast: Primary : Secondary : Tertiary : Quaternary • Morphology • Focal vs. Diffuse • Severity • Mild vs. Moderate vs. Severe
Causes of TBI • Civilian TBI causes varies with age
Initial severity and outcome • Dikmen et al. (1995) Relative to general trauma controls, TBI associated with poor cognitive performance • In particular: attention, memory, processing speed • At 1 year post injury, those with less than 1 hr TFC performed similar to controls, 1-24hrs impaired in attention and memory, longer had more global impairments. • Zatick et al. (2011) also showed worse injuries associated with worse outcome and better recovery for milder deficits. • Roozenbeek (2012): 39274 patients: age, GCS motor score, and pupillary reactivity strongly predict 6mos outcome.
Predictors of good outcome • More education is correlated with good prognosis (Kreutzer et al., 1993) and premorbid cognitive function (Hanks et al., 1999). • Perhaps due to cognitive reserve (Satz et al., 1993; Stern et al., 2006) • Generally, severe symptoms predict poor outcome • Low GCS, long PTA and LOC, brain imaging findings, dural penetration, pupillary abnormalities, hypoxia, systemic complications • Acute neuropsychological results is a better predictor than neurological severity (Hanks et al., 2008)
Recovery from mild TBI • Numerous studies suggest mild TBI typically resolves <3 months without treatment (Dikmen et al., 1986; Dikmen et al., 2001; Levin et al., 1987; Barth et al., 1989; Macciocchi et al., 1996; McCrea et al. 2003) • 90% spontaneous recovery • 10% persistent symptoms, include dizziness, headaches, pain, fatigue, depression, return to work. If complicated mTBI, ‘post concussive syndrome’.
Recovery from Moderate/Severe TBI • Millis et al. (2001) tracked 182 individuals 5 years post injury • 22% improved, 63% unchanged, 15% declined • Improvement in processing speed, visuoconstruction, verbal memory • Dikmen et al. (1995) 1yr post injury, more severe TBI were 25 percentile points lower than trauma controls. • Salmond et al. (2005) more severe TBI impaired in attention, verbal learning & reaction time, but spared spatial working memory. • Not all cognitive deficits are organic: medication, depression and premorbid factors contribute.
Gender • TBI more frequent in men then women • Iverson et al. (2011) study of 11951 men and 654 women with TBI from Afghanistan/Iraq • PTSD most common, women relatively less • Depression common, women x2 more • Anxiety disorders, women x1.3 more • Type of TBI (e.g. blast) might explain some of these differences
Genetics • APoE 4 associated with Alzheimers Disease (independent of TBI). • APoE 4 and recurrent TBI have cognitive and dementia risks (see sports literature: Jordan et al., 1997; Kutner et al., 2000). • Impact on single TBI remains controversial • Teasdale (2005). Large study (1094 patients, 513 with mTBI) showed no difference at 6 mos. However, potential interaction such that pediatric TBI with APoE 4 had worse outcome
Pediatric TBI • Giza (2006) review notes differences • Pediatric skull thinner, more pliable • Larger head relative to body, less developed neck muscles • Different causes (pediatric falls) • Higher blood flow, higher metabolism • Higher incidence of post traumatic epilepsy • Interfere with developmental potential • Calcium influx more diffuse in children (see cascade slides) • Young brain more vulnerable to excitotoxic injury • Treatment: education of caregivers (parents, teachers); continuous assessment (skills may not have yet developed).
Elderly TBI • Roe et al. (2013) examined severe Norwegian TBI in adults vs elderly. • Elderly more likely to have suffered falls • Hematoma more common • Dura sticks to skull, anticoagulants common • 25% of adults and 66% of elderly died within 3 mos. • Adults more likely to be inpatients and go to rehab units. • No difference in functional outcome at 3 mos. • Clinically: Work rehab not as important, since there is less recovery, educate caregivers.
Pause • Break
Military Traumatic Brain Injury • Brain related problems major issue for military • Incidence and Financial Costs • Reasons for high incidence • Blast Induced Neuro Trauma • Gunshot wounds • Resources • http://www.dvbic.org/resources • http://www.gvsu.edu/veteranstbi/ ($)
War related injuries • In Vietnam, wounded: killed was 2.6:1 • In Iraq/Afghanistan the ratio is 16:1 • Radically improved acute care • Embedded medics • New training and medical equipment • decompressive craniotomy common for evacuation (ICP) • New body armor • Different type of injury (in Iraq/Afghanistan, typically blast) • Low rate of injury means ability to provide maximal acute care (e.g. no triage) • Clear long-term obligations for care
US Health Care Costs • US spends disproportionate amount on health care. • Yet, 48m US citizens do not have health care
VA Budget Rising cost of military medicine • DoD health care costs rose from $19bn in 2001 to $49.4bn in 2014. • VA 2014 Budget rose from $48.7bn in 2001 to $152.7 billion in 2014
Mental Disorders in US Military • Mental disorders largest and fastest growing military hospitalization • Not only TBI: 20% from Iraq/Afghanistan report PTSD/depression.
Military TBI • Higher incidence (better awareness?)
Incidence by severity • Increase appears to be in mild TBI • Better identification? • Are ‘mild’ blast TBIs similar to other mild TBIs?
3.2% Military TBI • approximately 80% of service members TBIs occur in a non-deployed setting. • Common causes of TBI include vehicle crashes, falls, sports and recreation activities, and military training. • 77% mild TBI
Civilian vs Military TBI • Blast TBI signature injury from current wars. 68% injured in combat have blast injuries Civilian Causes Vary With Age
TBI in the military • TBI incidence for 1.6m deployed to Afghanistan/Iraq • ~1800 penetrating wounds. • 66% of all wounded soldiers that do not return immediately to service have TBIs. • Total combat TBI rates vary between sources • ~10,000 blast injuries (assuming 85% have closed head injuries) • ~30% of troops who have been at the front for >4 months at risk from blast injury.
Blast Induced Neuro Trauma • Blast leading cause of injury/death in Iraq • 69.4% of wounded caused by explosion • 62% of blast injuries result in TBI • 85% of TBIs are closed head
Blast Injury • Primary Blast Injury: blast pressure wave[s] • Secondary Blast Injury: Sharpnel stiking victim • e.g. penetrating injury • Tertiary Blast Injury: Victim hitting objects • Closed or open head injury • Quaternary Blast Injury: Other • Include flash burns, crush and respiratory injuries, psychological consequences • NB: Primary, Secondary and Tertiary Blast Injuries can each cause primary or secondary brian injuries.
BINT Consequences • Cernak and Noble-Haeusslein (2010): Despite similar secondary injury cascades, BINT has characteristics not seen in other types of brain injury • weight loss • hormone imbalance • chronic fatigue • headache • problems in memory, speech and balance
Blast injuries • MacDonald et al. (2011) examined 21 controls and 63 soldiers with blast related mTBI (no injury detected with CT), DTI within 90 days of injury. (47 followed up 6-12 months later) • Reduced white matter near Cerebellum, Cingulate, Orbitofrontal cortex.
Blast Induced Neurotrauma (BINT) • BINT signature injury of recent wars • Overpressure has dramatic effects on gas-containing organs (lungs, ears). • Brain mostly liquid/solid and not compressible (Monro-Kellie doctrine). • Both initial pressure wave and reflections can cause injury. • Scott et al. (2006): Military blast associated with Hearing loss (42%), eye injuries (26%), brain injuries (66%), abdominal injuries (22%) and stress syndromes.
Blast injury • Lu et al. (2012) exposed monkeys to blast injuries. Histology at 3 days or 1 mos post injury • Behaviorally: working memory and motor impairments • Purkinje neurons in the cerebellum and pyramidal neurons in the hippocampus • White matter injury to myelinated axons. Apoptosis of astrocytes.