Download

1 / 68
680 likes | 1.09k Views
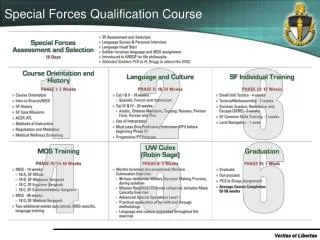
Special Forces Medical Sergeants Surgical Training. Rick Kelly, SFC/18D (Ret), GS-11 Primary Instructor for Surgery SFMS, SARR Joint Special Operations Medical Training Center (JSOMTC). DISCLAIMER.

E N D
Special Forces Medical Sergeants Surgical Training Rick Kelly, SFC/18D (Ret), GS-11 Primary Instructor for Surgery SFMS, SARR Joint Special Operations Medical Training Center (JSOMTC)
DISCLAIMER • The opinions and/or assertions contained herein are the private views of the author and are not to be construed as official nor as reflecting the view of USSOCOM, SWMG(A), the Department of the Army or the Department of Defense . • Financial disclosures: None. • The presenter will not discuss patients or wounds mentioned in this presentation beyond what is presented.
Objective • My intent is to enlighten the many health care providers that have the opportunity to advise and support Special Forces Medics, in order to reduce misunderstandings and confusion when providing this needed support. By understanding what the Special Forces medic is taught and why, you will better understand how to assist him.
AUSTERE vs. AUSTERE Military medical units vs. International Committee of the Red Cross (ICRC) and SF Medics
AUSTERE (Military) • We know that the conditions a Forward Surgical Team works under is much more challenging that working in a fixed treatment facility • The Forward Surgical Team does have many luxuries that the 18D does not have • This is rightfully so, our troops deserve the best forward medical treatment in the world
AUSTERE International Committee of the Red Cross(ICRC) • The ICRC has been highly successful without many of the luxuries that an American Forward Surgical Team has • Without these luxuries, the ICRC have found a way to be successful • 18D’s will be working in conditions much more aligned with the ICRC
Why we have adopted the ICRC Military Medicine Triad vs. Equipment (resources) Evidence vs. Environment The ICRC has abundantevidence of success, working in the environment and with resources similar to the 18D
Topics • Background • What we learned • What we teach and why
Single Slide on Anesthesia • Monitored Anesthesia Care • Light sedation • Regional Nerve Blocks • Sciatic • Femoral • Posterior approach to the inner scalene • All associated lower blocks • IV Ketamine bumps, or drips (TIVA) with a Benzo for failed blocks • Back to the good stuff…
Background • NATO Emergency War Surgery • Introduction of ICRC methods • Abandonment of ICRC methods • Procedures performed as in Military MTF • Reintroduction of ICRC methods
Background • What we teach now • Wound excision • Closure (DPC, Secondary) • Fasciotomy (lower leg, forearm) • Amputation • Conditions they perform under now • Only the items in their Tactical Medical set • Only with the personnel that they will have • 2 medics, one or two team mates.
Facts • The 18D who receive war wounded Pts (often wounds a day or two old) will sometimesbe, not only the prolonged-care provider but, the definitive care provider • Conventional techniques are BY FAR a better way to treat these types of injuries. They preserve function better by retaining more tissue, with less scarring, in addition to decreasing pain and healing times in situations that: • Are relatively clean • Time is available • Manpower is available • Supplies are available • The 18D israrely, if ever, be afforded such luxuries
What We Learned • During ourconventional way of performing surgery • Full OR staff • High-tech, power-hungryequipment • Wounds • Relatively clean wounds • Visited surgically within 1 hour of injury • Resulted in extremely high post-op infection rates • 2 things that we immediately changed were • Discontinue electric cautery • Discontinue high pressure pulsatile lavage
What We Learned • ICRC method • 1 medic “surgeon,” 1 medic anesthesia, 1 or 2 “helpers” • Equipment inherent to the 18D TAC sets • Wounds • Extremely contaminated • Wounds visited surgically after 24 hours • Immediate and dramatic drop in post-op infection rates
JSOMTC Infection Rates, using Conventional Methods • Generally 30%-50% • Some attributed to leaving vulnerable tissue in the wound • Wound not “matured” • Cautery, high-pressure pulsatile irrigation • Separating involved (injured) muscles was not emphasized • The surgical technique and the treatment of tissues • We now stress the importance of gentle treatment of the viable tissue which will remain in the wound • The biggest culprit likelythe daily “wet to dry” dressing changes • Dressing changes in an austere environment (even if the dressing directly covering the wound remains) leaves tissues in or adjacent to the wound to collect contaminants which will grow and invade the wound
JSOMTC Infection Rates, using ICRC Method • Approximately 1% • Almost all can be attributed to having the bandage come off the wound prior to DPC or the bandage gets saturated with water • Either by mistake or purposeful • Very small percent due to missing something during excision or not incising long enough (tension) • Not separating involved muscles to determine the full extent of the injury • An extremely small percent post-closure due to closure under tension
ICRC Doctor Robin Coupland Anecdote • Dr. Robin Coupland gave an example of a conflict in which the important people had their wounds tended to daily and the unimportant people were left forgotten in the bowels of the ward. The ones which were tended to daily suffered great infection, but for the ones which were forgotten about, their wounds healed fine.
What we Teach and Why • So as I continue, you may scratch your heads and think that something is amiss. I cordially and enthusiastically invite any and all to come visit us and witness for yourselves what we do, what we do it with, how we do it and the results that we get. I believe that we will make a believer out of you, as the many providers who have personally witnessed what we do in our ORs.
ICRC References • Designed to help surgeons and non-surgical physicians to understand the nature of the injuries encountered and the medical working environment in a war-torn country • The ICRC has been successfully been treating patients under these conditions for decades – they literally wrote the book(s) on it! • This is exactly what we are expecting from our Special Forces Medics • Many of the .pdf versions are free to download in multiple languages
What We Teach and Why Reference: War Wounds of Limbs: Surgical Management, Coupland, ICRC 2008, first print 1993
What We Teach and Why Reference: War Surgery: Working with Limited Resources in Armed Conflict and Other Situations of Violence, Vol. 1, C. Giannou, M. Baldan, ICRC, May 2010 Available for free download: https://shop.icrc.org/reference-publications-military.html
What We Teach and Why Reference: War Surgery: Working with Limited Resources in Armed Conflict and Other Situations of Violence, Vol. 2, C. Giannou, M. Baldan, A. Molde, ICRC, March 2013 Available for free download: https://shop.icrc.org/reference-publications-military.html
What We Teach and Why • 11.5 hours of surgery lecture • 9 hours of surgery demonstration • 4 days of wound-excision practical exercise • 4 days of wound-closure practical exercise • 4 days of amputation/fasciotomy practical exercise • We teach the ICRC method of amputation and the standard2-incision, 4-compartment release of the lower leg and forearm, as advocated by the USAISR, so we will not go into these details in this presentation • 24/7 nursing care for the entire 12 training days by the students • Telemedical consults also available 24/7, via on-call instructors
What we Teach and Why • Why the ICRC method works for us • Easy to understand references • Basics, basics, basics… oh yeah, did I say basics? • We take young, but talented enlisted men: • give them an old, contaminated and even infected wounds • give them only the bare and crude necessities to perform the procedure • A few instruments • 4x8 gauze packs • Cloth drapes • They sterilize in a pressure cooker or use formaldehyde or gluteraldehyde • Give them non-compliant patients that live in filth • Allow the students to make all the treatment decisions and plans • With all this, these medics are HIGHLY successful!
Average SF Medic Surgical Pack Emesis basin 4x8 gauze Hand towels/sterile wraps (draping material) Volkmann retractors Lewis rasp Gigli saw/handles Adson forceps Tissue forceps Needle drivers Mayo dissecting scissors General operating scissors #3 scalpel handle/#10 surgical blade Allis forceps (for both procedure and as use as sponge forceps) Hemostats Towel clamps
What We Teach and Why • Who are these soldiers? • They are extremely well trained Special Forces Medical Sergeants • They are not medics whose primary mission is to provide medical care • They are NOT Civil Affairs medics, Psyops medics, JSOC medics, infantry medics, etc. • These men are a part of a small team whose primary mission is the planning and performance of full-spectrum combat and combat-related missions • Their mission set dictates their time utilization • This is but one constraint…
SF often work in split teamsor cells in which eachindividual is needed for a successful combat mission
What We Teach and Why • What are some other constraints? • Supplies • A team usually deploys with a pallet, sometimes 2, depending on the mission • This pallet space is shared with personal gear, weapons systems, demolition and ammo, communications equipment, other tools needed for the mission, food, and other miscellaneous stuff as well as the medical gear • Resupply may or may not be available when needed, especially in the amounts needed • Manpower • There are only 2 qualified medics on a detachment (at best). • Other detachment members have limited medical knowledge • Cross training is dependent on the medic and time available
Medical Equipment Loadout Team Loadout Typical space for medical equipment
Surgical Debridement or Amputation (sterilization takes over 2 hours) Sterile Surge pack 4 Chlorhex scrubbers 2 Surg Masks 2 Surg Caps 2 Gowns 2 Double sets of gloves 2 Sterile scalpel blades 1 Sterile Coban 4 plastic Steri drapes 2 suture packs 2 ligature packs Sterile rubber bands Compression Socks Casting/padding material Sterile Surge pack 4 Chlorhex scrubbers 2 Surg Masks 2 Surg Caps 2 Gowns 2 Double sets of gloves 2 Sterile scalpel blades 1 Sterile Coban 4 plastic Steri drapes 2 suture packs 2 ligature packs Sterile rubber bands Compression Socks Casting/padding material Delayed Primary Closure 4-7days after insult
Supplies Twice daily dressing changes x 6 days for 1 patient (Does not include fluids nor drugs)
Medical Waste is a Concern in Some Environments Twice-daily dressing changes x 6 days for 1 patient (Does not include fluids nor drugs)
Medical waste in a non-permissive environment with near-peer competitor? Probably not feasible
Man-Hours Needed Initial procedure takes about 10 man-hours total • 1 Hour Initial Assessment • 2 Hours Manual Labs to ensure patient stable– Hematocrit, Platelets, WBC Plus… Each Subsequent Procedure takes another 6-7 man hours • 2 Hours for equipment cleaning and sterilization • 1 Hour for pre-anesthetic exam • 1 Hour for equipment layout and room prep • 1 Hour for pre-procedure sedation/regional anesthesia • 1 Hour for procedure • 1 hour (minimum) for post-op monitoring
What We Teach and Why • What does this mean? • It means that even when the SF medic exercises economy of time, supplies and motion, conventional treatments will still overtax the medics situation and probably have an unsuccessful outcome • These men will be performing trulyaustere medicine; not just operating in austere country • They perform these procedures to save lives and limbs; usually on old, mismanaged or neglected wounds of indigenous people • Often the definitive provider
Sweetwater Resort Turned Aid StationHMC Lust (Subic Bay, Philippines)
HMC Lust (Jolo, Philippines)April 2014 - 81 Patients Over 6 MASCAL Events
Serial Debridement • Although the ICRC does mention serial debridement in their references, they (the ICRC) do not normally practice this technique because of: • Time • Supplies • Manpower • For the same reasons as the ICRC, we do not recommend this technique for the SF Medic, unless: • He knows for a fact that this casualty will be in the hands of a qualified surgeon within a day or two
Wound Excision Antibiotics No S/SX Infection S/SX Infection Secondary intent if later than 7 days post injury DPC 4-7 days after injury Redebridement DPC if done within 7 days of injury DPC performed but closure becomes infected At DPC, the wound is infected Redebrideprn/pulse irrigation Antibiotics Infrequent dressing change (Q 4-5 days) (secondary intent) In the OR remove sutures, redebrideprn, Signs/Symptoms of infection Yes No Continue infrequent dressings Daily sugar or honey dressings Not effective Effective Continue sugar or honey dressings or convert to infrequent dressings Antibiotics Redebrideprn/pulse irrigation
ICRC Principles • Surgical treatment of war wounds is completed in 2 stages • Wound excision – leaving the wound open • Delayed primary closure or closure by secondary intent
ICRC Principles • Basic Principles • Stop hemorrhage and maintain hemorrhage control • Make adequate skin and fascial incisions • Decompression • Drainage • Exposure • Remove culture medium • Leave the wound open • To decompress • To drain • Re-establish physiological function • Handle tissue gently and treat the tissues with respect • Do not create culture medium