Download
1 / 1
10 likes | 177 Views
Fabry disease in donor kidneys with 3 and 12 years follow-up after transplantation. Willy Aasebø 1 , Erik H. Strøm 2 , Torstein Hovig 2 , Liv H. Undset 1 Arvid Heiberg 3 , Trond Jenssen 1,4.

E N D
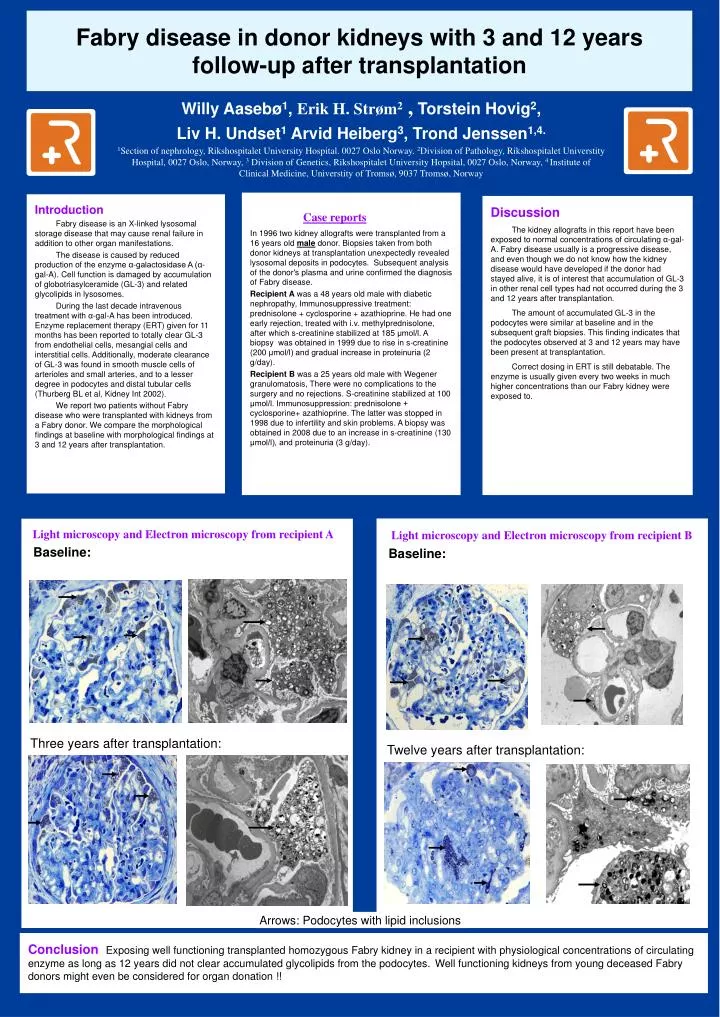
Fabry disease in donor kidneys with 3 and 12 years follow-up after transplantation Willy Aasebø1, Erik H. Strøm2 , Torstein Hovig2, Liv H. Undset1 Arvid Heiberg3, Trond Jenssen1,4. 1Section of nephrology, Rikshospitalet University Hospital. 0027 Oslo Norway. 2Division of Pathology, Rikshospitalet Universtity Hospital, 0027 Oslo, Norway, 3 Division of Genetics, Rikshospitalet University Hopsital, 0027 Oslo, Norway, 4 Institute of Clinical Medicine, Universtity of Tromsø, 9037 Tromsø, Norway Case reports In 1996 two kidney allografts were transplanted from a 16 years old maledonor. Biopsies taken from both donor kidneys at transplantation unexpectedly revealed lysosomal deposits in podocytes. Subsequent analysis of the donor's plasma and urine confirmed the diagnosis of Fabry disease. Recipient A was a 48 years old male with diabetic nephropathy, Immunosuppressive treatment: prednisolone + cyclosporine + azathioprine. He had one early rejection, treated with i.v. methylprednisolone, after which s-creatinine stabilized at 185 μmol/l. A biopsy was obtained in 1999 due to rise in s-creatinine (200 μmol/l) and gradual increase in proteinuria (2 g/day). Recipient B was a 25 years old male with Wegener granulomatosis, There were no complications to the surgery and no rejections. S-creatinine stabilized at 100 μmol/l. Immunosuppression: prednisolone + cyclosporine+ azathioprine. The latter was stopped in 1998 due to infertility and skin problems. A biopsy was obtained in 2008 due to an increase in s-creatinine (130 μmol/l), and proteinuria (3 g/day). Introduction Fabry disease is an X-linked lysosomal storage disease that may cause renal failure in addition to other organ manifestations. The disease is caused by reduced production of the enzyme α-galactosidase A (α-gal-A). Cell function is damaged by accumulation of globotriasylceramide (GL-3) and related glycolipids in lysosomes. During the last decade intravenous treatment with α-gal-A has been introduced. Enzyme replacement therapy (ERT) given for 11 months has been reported to totally clear GL-3 from endothelial cells, mesangial cells and interstitial cells. Additionally, moderate clearance of GL-3 was found in smooth muscle cells of arterioles and small arteries, and to a lesser degree in podocytes and distal tubular cells (Thurberg BL et al, Kidney Int 2002). We report two patients without Fabry disease who were transplanted with kidneys from a Fabry donor. We compare the morphological findings at baseline with morphological findings at 3 and 12 years after transplantation. Discussion The kidney allografts in this report have been exposed to normal concentrations of circulating α-gal-A. Fabry disease usually is a progressive disease, and even though we do not know how the kidney disease would have developed if the donor had stayed alive, it is of interest that accumulation of GL-3 in other renal cell types had not occurred during the 3 and 12 years after transplantation. The amount of accumulated GL-3 in the podocytes were similar at baseline and in the subsequent graft biopsies. This finding indicates that the podocytes observed at 3 and 12 years may have been present at transplantation. Correct dosing in ERT is still debatable. The enzyme is usually given every two weeks in much higher concentrations than our Fabry kidney were exposed to. Light microscopy and Electron microscopy from recipient B Baseline: Light microscopy and Electron microscopy from recipient A Baseline: Three years after transplantation: Twelve years after transplantation: Arrows: Podocytes with lipid inclusions Conclusion Exposing well functioning transplanted homozygous Fabry kidney in a recipient with physiological concentrations of circulating enzyme as long as 12 years did not clear accumulated glycolipids from the podocytes.Well functioning kidneys from young deceased Fabry donors might even be considered for organ donation !!