Download
1 / 24
240 likes | 275 Views
Explore the classifications and pathophysiology of immune hypersensitivity disorders including hypersensitivity, autoimmune, and immunodeficiency disorders. Learn about types I-IV hypersensitivity reactions, allergic disorders, autoimmune diseases like lupus, and their clinical manifestations.

E N D
The Nature of DiseasePathology for the Health Professions Thomas H. McConnell Chapter 3 Disorders of the Immune System
Brief Review of Adaptive Immunity Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Overview of Immune Disorders • Immune disorders fall into 3 major categories: • Hypersensitivity disorders • Caused by an allergen (antigen causing an allergic resp.) • Allergic rhinitis, anaphylaxis • Autoimmune disorders • Immune system attacks self • RA, SLE • Immunodeficiency disorders • Absent or depressed immune response (primary; acquired) • DiGeorge syndrome, AIDS
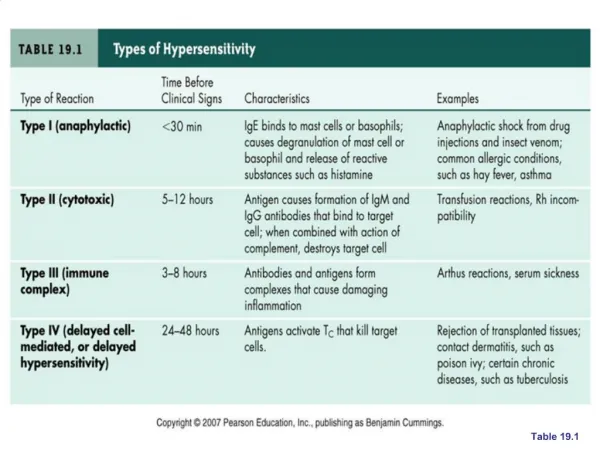
Hypersensitivity • Exaggerated immune response • Environmental or internal antigens • Associated more closely with certain HLA genotypes • Four types • Type I: immediate hypersensitivity (allergic; anaphylactic) [B cell] • Type II: cytotoxic hypersensitivity [B cell] • Type III: immune-complex hypersensitivity [B cell] • Type IV: cellular hypersensitivity (delayed) [T cell] • Mnemonics: ACID and AnGST
Type I (Immediate) Hypersensitivity Important points: - Immediate (after initial sensitization) - Antigen is extrinsic (foreign) - Local or systemic - B cell (ab) mediated - IgE - Mast cells (histamine; other mediators) - Examples - Allergic rhinitis (seasonal = hay fever) - Anaphylaxis (local or systemic) - One form of latex allergy (to the latex itself) Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Type II (Cytotoxic) Hypersensitivity Important points: - Usually immediate (> sensitization) - Ag is extrinsic or intrinsic - May be initiated by a hapten - Local or systemic - B cell (ab) mediated - IgG or IgM - Ab attach to cell surface - Cell injury from: - Complement - NK Cell, phagocytes (ADCC) - Altered cell function - Examples - Txfusion Rexn - Grave’s Disease - Myasthenia Gravis - Autoimmune hemolytic anemia Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Type III (Immune Complex) Hypersensitivity Important points: - Usually immediate (> sensitization) - Antigen not fixed in tissue - Local or systemic hypersensitivity - B cell (ab) mediated - IgG or IgM - Damage from ag-ab complexes - Examples - SLE - Serum sickness - Farmer’s Lung - One form of latex allergy (to the latex itself) Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Type IV (Delayed Type) Hypersensitivity Important points: - Delay (28-48 hrs) - T cell mediated - Damage from TCTL attack - Examples - TB - Transplant rejection - Contact dermatitis (poison ivy) - Latex allergy (to chemicals used) - Granulomatous inflammation - Rheumatoid arthritis - Multiple sclerosis - Type I Diabetes Mellitus Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Allergic Disorders and Atopy • Allergy: Exaggerated, but otherwise normal immune response to foreign antigen (regardless of the type of hypersensitivity response) • Allergen: an inciting foreign substance • Atopy: allergy due to type I hypersensitivity • Common • Usually affect: nose, skin, and airways (-> atopic triad: rhinitis, dermatitis, asthma • Strong familial (genetic) tendency • Pathophysiology is from IgE-sensitized mast cells • Food allergies (infants: milk, soy, eggs, peanuts, wheat; adults: usually nuts and seafood) • Anaphylaxis
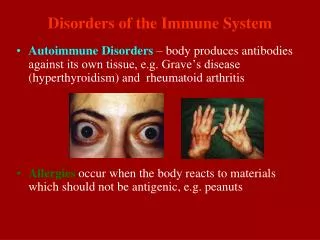
Autoimmune Disorders • Self antigens become targets of the immune system • Affects ~ 2% of US population; autoimmune ab common, especially in elderly • Clinical manifestations are extremely varied • Genetic susceptibility, e.g., HLA-B27 and rheumatoid disease • Some hypothesized causes: • Imperfect T and B cell programming • Inaccessible self-antigens that become exposed for the first time to the immune system • Molecular mimicry • antigenic determinants of an infectious agent or foreign protein may be shared with self antigens • Ab produced by B cells cross-react with self antigens • Infection and inflammation
Systemic Lupus Erythematosus (SLE) • Chronic inflammatory, rheumatic, autoimmune disease characterized by remissions and exacerbations • Etiology unknown (UV?, genetic?, hormonal?) • Leukemia and renal failure usually major cause of death • Classifications • Systemic lupus - involvement of 1 or more of these systems: Musculoskeletal, Lungs, Kidneys, CNS, CVS, hematological • Discoid lupus - limited to skin involvement • Drug-induced lupus – procainamide, hydralazine, isoniazid • Pathophysiology • Anti-DNA/RNA (antinuclear) autoantibodies produced by hyperactive B cells • Detection test is very sensitive, but not very specific • Other autoantibodies against RBCs, platelets, lymphocytes • Autoantibodies+antigens -> Type III immune complex disease • IC cause vasculitis with inflammation and necrosis
Systemic Lupus Erythematosus (SLE) Malar (“butterfly” ) phtotsensitive rash Figures from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Scleroderma (Systemic Sclerosis) • Pathophysiology • Etiology unknown (genetic?, immune?, environmental?) • Microvascular damage, inflammation, *fibrosis of interstitium • Many organs can be affected, especially the dermis • Types of scleroderma • Systemic sclerosis • CREST syndrome • Calcinosis • Raynaud’s phenomenon • Esophageal dysfunction • Sclerodactyly • Telangiectasis • Localized or limited; skin on fingers, hands, and face (better prognosis)
Amyloidosis • Amyloid – mixture of insoluble, mis-folded, crystalline proteins; some may be Ig fragments • Amyloidosis – Any dysfunction resulting from deposition of amyloid protein • Examples: • Light chain amyloidosis (in B cell malignancies) • Reactive systemic (with chronic inflammatory disease) • Hereditary (primary) amyloidosis – caused by several gene defects, e.g., hereditary Mediterranean fever • Amyloidosis of aging • Islets of Langerhans (Type II diabetes) • Endocrine tumors (some) • Brains of patients with Alzheimer’s Disease Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Tissue Transplantation • Successful transplantation is highly dependent upon having as close a match as possible between tissue antigens (MHC/HLA and ABO) of donor and recipient • Except for an autograft, every transplant has a possibility of rejection; immunosuppressive therapy • Types of rejection (an immune reaction) • Hyperacute; minutes or hours due to preformed ab • Acute • most common and treatable • T and B cells involved • Rejection mediated by cellular immune response • Signs of inflammation with fever, redness, swelling, tenderness • Chronic; 4 months to years causes chronic vasculitis compromising blood flow to transplant
Graft versus Host Disease (GvHD) • Frequent and potentially fatal complication of bone marrow transplant • Immunocompetent cells of the donor recognize the recipient’s tissues as foreign • Cell-mediated response • Host is typically immunocompromised and unable to fight grafted cells’ attack • Other areas affected: skin and GI tract (lots of epithelial cells), liver • Acute GvHD: dermatitis, diarrhea, jaundice • Chronic GvHD: dermal sclerosis, Sjogren’s syndrome, immunodeficiency
Transfusion Reactions • Minimized by careful testing prior to transfusion: • Major crossmatch: donor RBCs with recipient plasma • Minor crossmatch: donor plasma with recipient RBCs • Two major types of transfusion reactions: • Major • Incompatible blood types • Recipient’s pre-existing ab hemolyzes of donor’s RBCs • Severe hemolysis, thrombosis, DIC, renal failure, death • Minor • Any rexn NOT potentially life-threatening • Fever, chills, back pain, hives, rash • Erythroblastosis Fetalis (hemolytic disease of the newborn) - mother generates anti-Rh antibodies against fetal RBCs
Immune Deficiencies • Failure of immune mechanisms of self-defense • Primary (congenital) immunodeficiency • Genetic anomaly • Secondary (acquired) immunodeficiency • Caused by another illness • Clinical presentation • Development of unusual or recurrent, severe infections (usually opportunistic infections) • T cell deficiencies • Viral, fungal, yeast, and atypical microorganisms • B cell and phagocyte deficiencies • Microorganisms requiring opsonization (bacteria, some viruses) • Complement deficiencies
Primary Immunodeficiencies • Affect the development of T and B cells • Isolated IgA deficiency (B cells) • Most common primary immunodeficiency • Recurrent infections of mucous membranes • X-linked agammaglobulinemia -Bruton Disease (B cells) • X-linked recessive defect of B cell development • Recurrent infections by about 6 months of age • Bronchitis, pneumonia, sinusitis, pharyngitis, otitis, GI infections • Intestinal parasites and certain viral infections • Thymic hypoplasia (DiGeorge syndrome) (T cells) • Deficient T cell function due to failure of thymus to develop • Area around thymus often affected: neck, face, ears, heart, aorta • Viral, fungal, protozoan infections • Severe combined immunodeficiency - SCID (B and T cells) • Lymphoid tissues and thymus underdeveloped; lack of functional immunity • Wide variety of infections before 6 months of age; total isolation required
Acquired Immunodeficiency Syndrome (AIDS) • By far most common cause of acquired (secondary) immunodeficiency • Follows infection with Human Immunodeficiency Virus (HIV-1 (US), HIV-2 (W. Africa)) • Humans are the only reservoir; no animal reservoir • Virus attaches to CD4 antigen of TH (and related macrophages) but must also use several other receptors (chemokine) to infect, i.e, CD4 is necessary but not sufficient for infection • Reverse Transcriptase (RT) allows the RNA genome to be ‘reverse’ transcribed into DNA, and the abnormal DNA is inserted into host genome • Corrupted cellular DNA produces new HIV RNA and virus particles • Virus particles exit dying cell to infect other cells Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Additional HIV/AIDS Terminology & Facts • Modes of transmission for HIV virus • Contact with infected blood or blood products during transfusion or transplantation • Contact with infected body fluids, e.g., semen, vaginal fluids • Across the placenta from infected mother to fetus • Although HIV is also found in saliva, urine, tears, and feces there’s no evidence of transmission through these fluids • Viral load - number of circulating HIV particles/ml (should be zero) • Opportunistic infection – Any infection resulting from a deficient immune system, i.e., patient is immunocompromised or immunosuppressed • Peripheral blood CD4+ TH cell counts are a reliable indicator about the progress of the disease; the lower the counts the more advanced the disease and the poorer the prognosis • Current treatment regimen (Highly Active Antiretroviral Therapy, HAART) has dramatically extended the life expectancy of HIV-infected patients
Phases of HIV Infection and AIDS Figure from: McConnell, The Nature of Disease, 2nd ed., Wolters Kluwer, 2014
Classification of HIV Infection/AIDS is complex * Category B symptomatic conditions are defined as symptomatic conditions occurring in an HIV-infected adolescent or adult that meet atleast one of the following criteria: • They are attributed to HIV infection or indicate a defect in cell-mediated immunity. • They are considered to have a clinical course or management that is complicated by HIV infection. # Category C AIDS Indicator conditions include: - Wasting syndrome caused by HIV (involuntary weight loss >10% of baseline body weight) associated with either chronic diarrhea (two or more loose stools per day for ≥1 month) or chronic weakness and documented fever for ≥1 month - A number of associated conditions, e.g., Bacterial pneumonia, recurrent (two or more episodes in 12 months); Candidiasis of the bronchi, trachea, or lungs; Candidiasis, esophageal; Cervical carcinoma, invasive, confirmed by biopsy; Coccidioidomycosis, disseminated or extrapulmonary; Encephalopathy, HIV-related; ,Kaposi sarcoma; Mycobacterium tuberculosis, pulmonary or extrapulmonary; Pneumocystisjiroveci (formerly carinii) pneumonia (PCP); Toxoplasmosis of brain Immunocompetent Immunosuppressed AIDS Table from: http://aidsetc.org/guide/hiv-classification-cdc-and-who-staging-systems