Download
1 / 32
320 likes | 730 Views
Angiomax (bivalirudin) in Peripheral Vascular Disease (PVD). Anticoagulation in PVD. Thrombus occurs in 100% of peripheral percutaneous intervention (PPI) cases Bleeding risks are greater in PPI than PCI PPI and PCI are different PPI requires superior anticoagulation.

E N D
Anticoagulation in PVD • Thrombus occurs in 100% of peripheral percutaneous intervention (PPI) cases • Bleeding risks are greater in PPI than PCI • PPI and PCI are different • PPI requires superior anticoagulation
Clinical Differences in PVD vs. PCI • Longer length diseased vessel • Larger sheath size requirement • Longer PTA/stented segments • Larger acute and chronic thrombus burden • Longer procedural times (sheath dwell times) • Multiple catheter, guidewire, devices, etc exchanges (oftentimes crossover techniques)
Clinical Differences in PVD vs. PCI (con’t) • “Low flow” state in peripheral versus coronary flow beds • Increased incidence of CRF (renal insufficiency) • Postprocedural anticoagulation (infrainguinal, limb salvage, ALI, etc.) • PVD- > 50-60% Diabetes: PCI- 20-30% Diabetes • PVD patients are hypercoaguable
Peripheral interventions • Percutaneous peripheral interventions (PPI) require predictable and reliable anticoagulation that also minimizes risk of bleeding • Large sheaths • Renal dysfunction • Long interventions • Strategies needed to improve throughput • Reduce time to sheath removal • Reduce time to ambulation • Heparin is typically used in PPI, but no data exist on the optimal level of anticoagulation • The limitations of heparin persist in PPI…
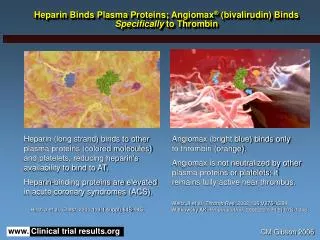
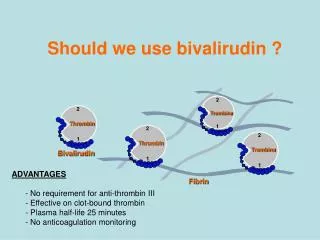
Bivalirudin in peripheral interventions • Bivalirudin: a thrombin-specific anticoagulant, superior efficacy, significantly less bleeding vs heparin in PTCA1 • Bivalirudin used in PPI registries: St Joseph’s, Naples Endovascular, Cardiovascular Institute of the South, Cardiovascular Research Foundation/Lenox Hill • Based on these limited data, bivalirudin may be an attractive alternative to heparin in peripheral interventions • May offer decreased vascular complications, earlier sheath removal time, earlier ambulation and decreased length of stay • Further studies are warranted 1Bittl et al AJC 2001
St. Joseph’s Hospital Registry Demographics • 72 Patients, elective procedures • 88 Lesions (4 with concomitant PCI) • Mean Age 65.8 yrs (Range 43-84) • 60% Male • 73% HTN • 23% Diabetes • Prior MI 25% • Prior PCI 62% • Prior CABG 27% • Prior CVA 10% Knopf et al, TCT 2002
St. Joseph’s Hospital Registry Methods • Bivalirudin bolus 0.75mg/kg in 100% • Infusion 1.75 mg/kg/hr used in 50% of cases • Mean ACT 286.6 (224-389) • Sheath 6F-11F • Mean creatinine pre 1.17 (0.7-2.7) • Plavix 99% • GP IIb/IIIa 0% • Closure devices 20% Knopf et al, TCT 2002
St. Joseph’s Hospital Registry Location of the 88 lesions • Iliac 33 • Renal 26 • Femoral 12 • Carotid 16 • Distal Aorta 1 • Subclavian 1 Knopf et al, TCT 2002
St. Joseph’s Hospital Registry Results • Success 100% • Bleeding 0% • Mortality 0% • Subacute closure 0% • Vascular repair 0% • CVA 0% • Post-procedure creatinine increase > 0.5 0% • Mean sheath removal 108 minutes • LOS 0.6 days (0-2) Knopf et al, TCT 2002
Naples Endovascular Registry 69 procedures Bivalirudin bolus 0.75mg/kg Infusion 1.75 mg/kg/hr Grubbs, CRT 2003
Naples Endovascular Registry Conclusions • Bivalirudin provided adequate anticoagulation for all • peripheral interventions • Achieved ACT targets immediately • No adverse events (bleeding, procedural failure, • acute thrombosis, or death) were seen. • Historical analysis of usual complication rates for this • composite set of procedures w/ heparin= 6% >1200 interventions. • Bivalirudin procedural success rate of 100% • on 12 consecutive arterial lysis cases is of note, • historical complete lysis rate of 78% in >100 cases using tPA • alone during the past 4 years. Grubbs, CRT 2003
Cardiovascular Research Fdn& LHH Carotid Stenting • 59 consecutive pts with bivalirudin (bolus 75mg/kg, 1.75 mg/kg/hr infusion throughout the procedure) • 83 case-matched controls with UFH (5,000U), same timeframe • mean age = 72 + 9 yrs • 60.4% male • No GP IIb/IIIa inhibitors • Neurological events, bleeding and vascular complications were recorded and adjudicated by an independent committee Adamyan et al, ACC 2003
B ivalirudin UFH P Clinical Outcomes n =59 n =83 value Death , n% 0 (/59) 0 (0/83) NS Major stroke, n% 0 (0/59) 1.2 (1/83) 1.00 Minor stroke, n% 0 (0/59) 0 (0/83) NS Hematoma > 5cm (%) 1.7 (1/59) 3.6(3/83) 0.64 Pseudoaneurysm(%) 0 (0/59) 2.4 (2/83) 0.51 Transfusion (%) 0 (0/59) 8.6 (7/81) 0.02 Vascular complication 1.7 (1/59) 4.9 (4/81) 0.39 Cardiovascular Research Fdn& LHH Results Adamyan et al, ACC 2003
Bivalirudin in peripheral interventions • Based on these limited data, bivalirudin may be an attractive alternative to heparin in peripheral interventions • May offer decreased vascular complications, earlier sheath removal time, earlier ambulation and decreased length of stay • Further studies are warranted
Direct Thrombin Inhibition in PVD Bivalirudin as Sole Anticoagulant in Peripheral Vascular Disease: A Safety and Feasible Alternative in Renal and Iliac Interventions David E. Allie, Mitchell D. Lirtzman, V. Antoine Keller, Mohamed H. Khan, Muhammad A. Khan, Peter S. Fail, Chris J. Hebert, Adam A. Allie, Craig M. Walker, Cardiovascular Institute of the South, LA, HCA, LA Allie et al ACC 2003
Bivalirudin as Anticoagulant Foundation in PVD: A Safety and Feasibility Study in Renal and Iliac PTA Design/ Methods • Retrospective, consecutive review of 180 renal, 75 iliac • Bivalirudin: 0.75 mg/kg bolus with 1.75 mg/kg/hr infusion for procedural duration • Variables: Sheath removal time (SRT), access complication (AC), time to ambulate (TA), and length of stay (LOS). • Follow up: 6 month renal and iliac duplex ultrasound and ankle-brachial index • Matched historical control with UFH Allie, ACC 2003
H istorical B ivalirudin C ontrol Variables P - value Renal, n=180 Renal, n=180 PPI Success, n (%) 180 (100) 179 (99) 0.31 73 AC (Major1), n (%) 2(1.1) 6 (3.3) 0.1532 AC (Minor2), n(%) 5(2.7) 8 (4.4) 0.3974 SRT <60 min, n (%) 152 (84) 106 (59) <0.0001 SRT >60 m in, n (%) 28 (16) 74 (41) <0.0001 LOS <24 hrs, n (%) 154(85.5) 130 (72) 0.002 LOS >24 hrs, n (%) 26(14.5) 50 (28) 0.002 TA <6 hrs, n (%) 136(75.5) 105 (58) 0.0005 TA >6 hrs, n (%) 44(24.5) 75 (42) 0.0005 Bivalirudin as Anticoagulant Foundation in PVD: A Safety and Feasibility Study in Renal and Iliac PTA Results: RT, LOS and TA all significantly shorter with bivalirudin 1="Major’ = any surgery, > 5 cm hematoma, or > 2u transfusion2="Minor’ = all other non-intracranial or retroperitoneal bleeding Allie, ACC 2003
B i va l irudin H istorical control Variables P - value Iliac n=75 Iliac n=75 PPI Success, n (%) 75 (100) 74 (98.6) 0.3173 AC (Major1), n (%) 2(2.5) 3 (4) 0.6503 AC (Minor2), n(%) 3(4) 5 (6.6) 0.4689 SRT <60 min, n (%) 36 (48) 21 (28) 0.0119 SRT >60 min, n (%) 39 (52) 54 (72) 0.0119 LOS <24 hrs, n (%) 42(56) 32 (43) 0.1036 LOS >24 hrs, n (%) 33(44) 43 (57) 0.1036 TA <6 hrs, n (%) 31(41) 19 (25) 0.0383 TA >6 hrs, n (%) 44(59) 56 (75) 0.0383 Bivalirudin as Anticoagulant Foundation in PVD: A Safety and Feasibility Study in Renal and Iliac PTA Results 1="Major’ = any surgery, > 5 cm hematoma, or > 2u transfusion2="Minor’ = all other non-intracranial or retroperitoneal bleeding Allie, ACC 2003
Bivalirudin as Anticoagulant Foundation in PVD: A Safety and Feasibility Study in Renal and Iliac PTA • Procedural success and clinical outcomes similar in both PVD groups with bivalirudin and UFH • Fewer access site complications in all groups Renal Iliac Bivalirudin UFH Bivalirudin UFH Overall 3.9% 7.7% 6.5% 10.6% Major 1.1% 3.3% 2.5% 4.0% Minor 2.7% 4.4% 4.0% 6.6% Overall Access Site Complications Bivalirudin = 3.8% UFH = 6.6%
Bivalirudin as Anticoagulant Foundation in PVD: A Safety and Feasibility Study in Renal and Iliac PTA • No thrombotic events, intracranial bleeding, or major surgical complications occurred in bivalirudin group • Sheath removal time, time to ambulation and length of stay were reduced compared to historical control • 6 month repeat PPI: • Renal 7/180 (3.9%) bivalirudin 8/180 (5%) UFH • Iliac and 3/75 (4%) bivalirudin 4/75 (5.3%) UFH Allie, ACC 2003
Direct Thrombin Inhibition in PVD • Principal Investigators: • David Allie MD Cardiovascular Institute of the South • Patrick Hall MD South Carolina Heart Center
Study Objective and Design • To demonstrate that Angiomax can safely replace unfractionated heparin as the primary anticoagulant in patients undergoing peripheral interventions, including outpatient interventions (<23hour) • Open label trial of Angiomax anticoagulation in renal, femoral, and Iliac lesions • 505 patients • 26 sites
Study Drug Administration • Angiomax 0.75 mg/kg IV bolus + 1.75 mg/kg-hr IV infusion for duration of procedure • GP IIb/IIIa’s at physician discretion • Bivalirudin post-procedural infusion 0.25 mg/kg/hr at physician discretion
Endpoints • Primary: Procedural success defined as ≤ 20% residual stenosis as determined by the treating physician. • Secondary: · Activated clotting times (ACTs) · Health economics (sheath size, time to sheath removal, time to ambulation, time to discharge, use of closure devices) · Death · Bleeding · Myocardial infarction (MI) · Unplanned revasc or surgical intervention for ischemia · Amputation · Renal function (relation to ischemic and bleeding outcomes).
Primary lesion/vessel • Renal n/N (%) 173/505 (34.3) • Iliac n/N (%) 140/505 (27.7) • Femoral n/N (%) 184/505 (36.4) • Other n/N (%) 8/505 (1.6)
Procedural characteristics • Clopidogrel pretreatment 95% • Aspirin 96.8% • GP IIb/IIIa inhibitors 4.4% • Procedural success 95%
Ischemic outcomes: 30 days * New Q-wave >0.04 sec duration in 2 or more contiguous leads
Summary: APPROVE 30-day outcomes • Bivalirudin, as the sole procedural anticoagulant, provided similar outcomes in all vessel types treated • Consistent anticoagulation at the dose tested • Major & minor hemorrhagic complications were low • Times to sheath removal, ambulation, and discharge were favorable and appear to increase the potential for same-day discharge without compromising efficacy or safety