Download
1 / 17
180 likes | 369 Views
Chapter 5 for 12 Lead Training -Making sense of the 12 Lead-. Ontario Base Hospital Group Education Subcommittee 2008. TIME IS MUSCLE. Making sense of the 12 Lead. REVIEWERS/CONTRIBUTORS Neil Freckleton, AEMCA, ACP Hamilton Base Hospital Jim Scott, AEMCA, PCP Sault Area Hospital

E N D
Chapter 5 for 12 Lead Training-Making sense of the 12 Lead- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE
Making sense of the 12 Lead REVIEWERS/CONTRIBUTORS Neil Freckleton, AEMCA, ACP Hamilton Base Hospital Jim Scott, AEMCA, PCP Sault Area Hospital Ed Ouston, AEMCA, ACP Ottawa Base Hospital Laura McCleary, AEMCA, ACP SOCPC Tim Dodd, AEMCA, ACP Hamilton Base Hospital Dr. Rick Verbeek, Medical Director SOCPC AUTHOR Greg Soto, BEd, BA, ACP Niagara Base Hospital 2008 Ontario Base Hospital Group
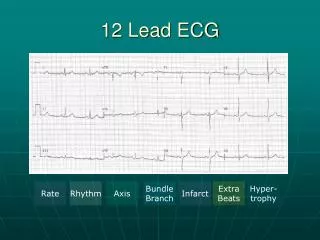
Chapter 5 Objectives • Describe how the ECG printout relates to time • Discuss the benefits and limitations of the machine analysis • Locate the isoelectric line using the calibration spike as a reference • Demonstrate how to validate a 12 Lead ECG
Machine Analysis • Machines analyze data for a conclusion • People interpret the electrocardiogram • Computer may give erroneous readings • Acute care providers must be able to tell the difference
Machine Analysis ****ACUTE MI**** • This statement is displayed by the machine when it determines the presence of ST elevation in accordance with it’s criteria. Local protocols must be followed upon seeing this message
Isoelectric Line • Basis for all voltage measurements • ST segment elevation/ depression measured from isoelectric line • Usually found at the bottom of calibration bar (arrow) • Best to measure from the TP Segment
12-Lead Validation • Lead I – P wave, QRS, and T wave is normally upright (positive) deflection • aVR – almost always downward (negative) deflection • Limb lead reversal can lead to an ECG misdiagnosis often referred to as “heart disease of electrocardiograph origin” • Can have significant impact on subsequent care of the patient
12-Lead Validation Normal • Lead I – upright • aVR - downward Lead I
12-Lead Validation RA/LA Reversed • Lead I – downward • aVR – upright Lead I aVR
START QUIT Well Done! Education Subcommittee