Download
1 / 43
440 likes | 805 Views
Cryptococcus neoformans and other Yeast. Dr Sharon Walmsley University Health Network Toronto. Organism. Encapsulated Heterobasidiomycetous fungi Asexual stage – simple narrow based budding Sexual – bipolar system, in-vitro 19 species. Identification. Routine laboratory media

E N D
Cryptococcus neoformans and other Yeast Dr Sharon Walmsley University Health Network Toronto
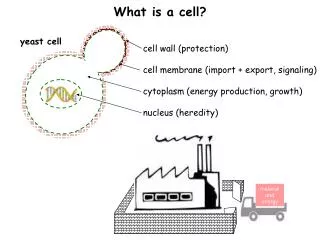
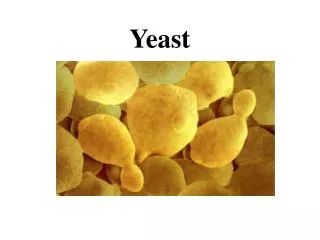
Organism • Encapsulated • Heterobasidiomycetous fungi • Asexual stage – simple narrow based budding • Sexual – bipolar system, in-vitro • 19 species
Identification • Routine laboratory media • 48-72 hours, 30-35ºC • May be inhibited by cycloheximide • White/cream opaque colonies which become mucoid with prolonged incubation
Rapid identification • India ink • Urease test (ureaammoniapH) • Laccase activity (diphenolic compoundsmelanin) – niger seed agar
Histopathology • Prominent capsule • Spherical narrow based budding yeast • May have hyphae or pseudohyphae • 5-10 mm diameter • 4 serotypes based on capsule
Ecology • Saprobe in nature – fruit, trees, rotting wood, soil • Bird guano – pigeons, turkey, chickens
Epidemiology • HIV • Lymphoproliferative disroders • Sarcoidosis • Corticosteroids • Hyper IgM or IgE syndrome • Monoclonal antibodies (infliximab) • SLE • CD4 T-cell lymphoma (idiopathic) • Diabetes • Organ transplant • Peritoneal dialysis • Cirrhosis • 20% without HIV have no underlying comorbidity
Spectrum of Disease Colonization Asymptomatic Disease
Rates of Disease Pre-AIDS .8/10 6/ year 1992 5/10 6/year HAART 1/10 6/year Africa/HIV 15-45%
Rates in Transplant • 18/100,000 • Increased with cell mediated immune inhibitors • Highest in kidney and liver • Rarely carried in through transplanted organ
Serotypes - Cryptococcus neoformans • A-D • Commercially available antibody tests • Biochemical tests • PCR
Serotypes - Cryptococcus neoformans Serotype A – 80% clinical cases B – tropical, subtropical – S. California, Hawaii, Brazil, Australia, SE Asia C – rare D – Europe – Denmark, Germany, Italy, France, Switzerland
Pathogenesis • Inhalation • Traumatic inoculation • Human – human – contaminated transplant tissue • Zoonosis?
Pathogenicity • Capsule – polysaccharide • Melanin • High temperature growth (37ºC)
Host Response • Cellular immune response, granulomatous inflammation • Th – 1 polarized • Cytokines – TNF, 1F-8, 1L-2 • Proinflammatory 1L-12, 1L-18, MCP-1, MIP • NK cells
Pathogenesis Host defense Size of Virulence of Inoculation strain
Clinical Manifestations Lung - Portal of entry - asymptomatic (1/3) life threatening pneumonia (ARDS) • Endobronchial colonization underlying chronic lung disease • Single pulmonary nodule • Symptomatic – acute, subacute
Clinical Manifestations CNS • Subacute meningitis or meningo-encephalitis • Headache, fever, cranial nerve palsies, lethargy, coma • Subacute (days) months HIV • Higher yeast burden • incidence raised intracranial pressure • Often disseminated • Immune reconstitution disease
Clinical Manifestations Skin • Papule with ulcerated center • Cellulitis, abscess • Rarely underlying bone lesions Prostrate • Asymptomatic (sanctuary) • Penile, vulvar lesions
Clinical Manifestations Eye • Ocular palsy, papilledema, optic neuritis • Retinal exudates +/- iritis • endophthalmitis
Diagnosis Microscopic • India Ink (50-80% + CSF) • Gram • Calcoflur white • Silver stain Culture • Blood agar • Routine blood culture
Diagnosis Serology • Latex agglutination, EIA, 90% sensitive & specific Radiology • CXR – infiltrates, nodules, lymphadenopathy, cavitation, effusion • CT/MRI – 50% normal, hydrocephalus, nodules
In vitro susceptibility testing • Low MICs – amphotericin, flucytosine, azole • High MICs – caspofungin • In vitro R demonstrated but most refractory cases are relapses
Therapy – Cryptococcal meningitis • Amphotericin B +/- flucytosine • Fluconazole • Amphotercin x 2 wk then fluconazole 400-800 mg/d x 8-10 wk • Chronic suppression fluconazole 200 mg/d
Raised ICP • CSF OP > 250mm • Rapidly progressive cerebral edema • Repeated LP, shunt • Corticosteroids not useful
Prognosis • Need to be able to control underlying disease • immunosuppression • prednisone • HAART • ? Adjunctive cytokines – interferon, GCSF
Poor prognosis • Burden of organism ( + India Ink, crypto Ag > 1:1024, poor CSF inflammatory response < 20 cells/uL) • Sensorium Mortality 10-25%
Prevention • Fluconazole prophylaxis • Active immunization- cryptococcal GXM-tetanus toxoid conjugate vaccine- in animal models, no human trials • Monoclonal antibodies- would require repeated injections • Avoid high risk environments
Cryptococcus neoformans (var gattii) • Initially described in Australia • Cultured from vegetation around river red gum trees, eucalyptus trees • Recent outbreak Vancouver Island
Cryptococcus neoformans var gatti • Outbreak Vancouver Island, January 02 • N = 59, 2 deaths
Cryptococcus neoformans var gatti • 75% primarily pulmonary disease • 25% CNS • 58% male, 5.3% Asian • Mean age 60 • Certain geographic locations • Never cultured from bird guano • May be associated with certain trees
C.gattiVancouver Island • 1999-2003 • 8.5 – 37/10⁶/year • Australia - endemic • 94 cases/million/year
C.gatti • Usually restricted to tropical, subtropical • Now in temperate zone • Able to identify an environmental reservoir • Identified in sea animals
Cryptococcus • Global epidemiology • Study – Canada 1984 • N = 78 • 7.7% C.gatti • 79.5% C.neoformans v grubii • 6.4% C.neoformans v neoformans (serotype D) • 6.4% C.neoformans v neoformans (hybid AD)