Download
1 / 30
330 likes | 647 Views
Diseases of the esophagus. Congenital: Atresia Traumatic: FB Caustic ingestion Perforation Neoplastic : Benign (rare) Malignant Functional : GERD Neuro-muscular : Achalasia. The most common; Atresia with Tracheo-esophageal fistula

E N D
Congenital: Atresia Traumatic: FB Caustic ingestion Perforation Neoplastic: Benign (rare) Malignant Functional: GERD Neuro-muscular: Achalasia
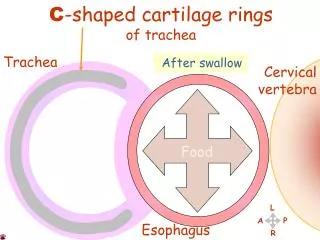
The most common; Atresia with Tracheo-esophageal fistula Regurgitation of food aspiration, chocking and cyanosis A catheter fail to enter the stomach Congenital Anomalies
طفل مولود كل مايرضع اللبن يرجع ويحصل له كحة شديدة واختناق وزرقان في اللون • نحاول نعدي قسطرة ماتعديش • (ممكن القسطرة تعدي tracheo-esophageal fistula only)) • Lipoidol swallow
The commonest congenital anomaly of the Esophagus The upper segment ends as a blind pouch The lower segment is connected to the trachea Atresia with Tracheo-esophageal fistula
Clinical Picture Immediately after birth: Marked regurgitation and Drolling Oral Catheter fails to enter the stomach Investigations; Lipidol swallow Treatment: Immediate surgical repair
Traumatic conditions 1- Foreign body 2- Caustic ingestion • Corrosive esophagitis • Stricture of the esophagus 3-Esophageal perforation
Children : the commonest . It is accidental عندما يلعب الطفل بوضع الأشياء في فمه Adult : suicidal Type of patient Type of foreign body Foreign Body in the esophagus In children: the commonest is coin & disc battery In adult: fish & meat bone In elderly : dentures and meat limp In suicisal cases: razor or pins
At the upper end: below the cricopharyngeal sphincter. The commonest site At normal constrictions Anywhere with sharp FB Type of patient Type of foreign body Site of impaction Sequlae: Mechanical obstruction dysphagia & regurgitation Disc batteries liquifactive necrosis and even perforation Sharp FB mucosal tears &even perforation
Type of patient • Type of foreign body • Site of impaction • Sequlae: • Symptoms • Signs • Investigations • Complications: perforation • Treatment : Removal by esophagoscope History Dysphagia It may be severe with drolling of saliva Regurgitation of undigested food
1- Foreign body 2- Caustic ingestion • Corrosive esophagitis • Stricture of the esophagus 3-Esophageal perforation
Corrosive esophagitis Etiology • Strong Alkalies(common) liquid cleaners &disc batteries progessive liquifactive necrosis and even perforation • Strong Acids: (rare) self limited coagulative necrosis act as a barrier protect the mucosa Symptoms: History: Severe mouth and throat pain Dysphagia: so severe , the patient cann’t swallow his saliva drolling Stridor and hoarsness: due to laryngeal edema ماب بطاريات
في الاسعافات الأولية يجب استخدام اشياء متوفرة حولنا Fist Aid : Combat shock ; IV fluids and analgesics Buffering solution: -Vinegar or diluted lemon to neutralize alkalies - Anti-acid for strong acids Emoluent solution; Egg white and milk to protect thr mucosa
Complications: Local: Perforation Healing by fibrosis stricture Systemic: - Dehydration &electrolyte disturbance - Scock: • Neurogenic due to pain • Hypovolaemic stricture
Treatment Analgesic Antibiotics Corticosteroids Nasogastric tube Endotracheal intubation or tracheostomy if indicated i.e if there is signs of respiratory obstruction
Etiology: healing of corrosive esophagitis by fibrosis Symptoms Signs: flexible esophagoscopy Investigations: Barium swallow Treatment: Permeable strictures Repeated dilatation through an esophagoscope Impermeble strictures colon bypass operation After a latent period of a few weeks - progressive dysphagia to solids then to fluids also - Regurgitation of undigested acid free food Stricture
Esophageal perforation Etiology: -Accidental: sharp FB or corrosives • Iatrogenic : unskilled esophgoscopy • هذه الحالة من الحالات الطارئة بحق ويجب تشخيصها والبدا في العلاج قبل مرور 24 ساعة حيث ان التأخر في التشخيص يزيد من نسبة الوفاة في هذه الحالات الي أكثر من 50% CORROSIVE
Sequlae: Clinically Investigations: Plain X ray: air in the neck, pleura, mediastinum Gastrografin swallow to detect the site and size of perforation Air in the neck surgical emphysema Air n the pleura pneumothorax Air in the mediastinum pneumo-mediastinum مريض بعد عمل منظار مرئ أو عنده جسم غريب The patient is feverish and toxic Dysphagia Hematemesis Retrosternal chest pain dyspnea
Treatment: In ICU في العناية المركزه Conservative: Nothing by mouth Massive antibiotic therapy Nasogastric tube in small perforation Gastrostomy in large perforation Surgical - Repair and, cervical or trans-thoracic drainage-
Incidence: The commonest malignant tumor of the esophagus Above 50 years old Commonly males Predisposing factors: - excessive tobacco & alcohol GERD Achalasia Plummer Vinson syndrome Esophageal carcinoma Koilonychia,, Angular stomatitis Glazed tongue
spines Spread Local: to surrounding structures: trache, bronchi, spines, recurrent laryngeal nerve Lymphatic: - Cervical part: to lower deep cervical LN • Thoracic part: mediastinal LN • Abdominal part: to coeliac LN Blood: trachea Late and Rare To Lung, Liver, Bone , Brain CT scan of the brain Abdominal ultrasound Bone scan Chet X Ray
مثال: رجل مدخن فوق الخمسين عنده صعوبة في البلع منذ شهرين تزيد باستمرار للأكل وبعد فترة اصبحت للأكل والسوائل مع فقدان واضح في الوزن In elderly patient commonly male: • Rapidly progressive dysphagia, first to solids then to solids & fluids • In large tumors : regurgitation of acid free food • Hematemsis & Melena • Later: hoarsness of voice • Loss of weight Symptoms Signs Investigations: • Barium swallow • CT scan • Biopsy • Metastatic work-up Treatment: Surgical resection followed by reconstruction and radiotherapy Prognosis is bad
Carcinoma of oesphagusThe stricture is -irregular -short -shouldering prestenotic dilatation is moderate هامة في العملي
Def Incidence Etiology: Deceases pressure of cardiac sphincter e.g in hiatus hernia Gastric hypersecretion: stess, smoking alcohol, caffiene, spicy foods, citrus frits Complications: esophagitis ulcer stricture Chronic pharyngitis & Laryngitis Cancer esophagus & Larynx Retrograde flow of gastric contents to the esophagus, pharynx and larynx due to frequent spontaneous relaxation of the cardiac sphincter Gastro-esophageal Reflux Disease GERD Above 40 Infants
GERD Symptoms: Esophageal; Retrosternal burning sensation (frequently absent) Pharyngeal: Throat irritation hmemming & Hawking to clear the throat نحنحه وتنخيم Laryngeal: Chronic irritative cough, hoarsness of voice, In infants , nocturnal laryngeal irritation laryngismus stridulus Signs: -esophagitis -ulcer May be stricture Investigations: 24 hours double probe(esophageal & pharyngeal) ph monitoring Measure the time the Ph is less than 4 It is diagnostic if the time is more than 5%
Treatment of GERD: Live style support -weight reduction Avoid smoking and foods that worsen symptoms Avoid lying down for 3 hours after a meal. Raise the head of your bed 6 to 8 inches Medical treatment: Anti-acidsto relieve heartburn H2 blockers, such as cimetidinedecrease acid production Proton pump inhibitors e.g omeprazole decrease acid production Prokinetics help strengthen the LES and make the stomach empty faster metoclopramide (Reglan). Surgical: After failure of medical treatment Fundoplication operation the upper part of the stomach is wrapped around the LES to strengthen the sphincter, prevent acid reflux, and repair a hiatal hernia. تغيير نمط الحياه مهم جدا لعلاجهذه الحالة انقاص الوزن تجنب التدخين و الاطعمة التي تزيد من الحموضة تناول طعام العشاء قبل 2-3ساعات من النوم النوم علي مخدة عالية أو رفع رأس السرير
Incidence; commonly middle aged neurotic female Etiology: Degeneration of ganglion cells of Auerbach’s plexus (parasympathetic) in the wall of the esophagus Failure of relaxation of the cardiac sphincter during swallowing marked dilatation of the lower two thirds of the esophagus Achalasia of the cardia Marked Dilatation of the lower two thirds esophagus above the cardia Failure of relaxation of Cardiac sphincter
Symptoms: Dysphagia: more to fluids Why? Regurgitation of undigested acid free food No loss of weightWhy? Signs: Excessive food stagnation المرئ مليان أكل غير مهضوم Marked dilatation ……. Investigations Barium swallow Manometric study: increase pressure of the lower segment Swalowing of fluids needs highly co-ordinated act of swallowing Solids can descend by gravity Because dysphagia is intermittent Marked dilatation of the lower 2/3 of the esophagus (segmoid esophagus) Tapering of the lower end
Treatment: • Conservative: Muscle relaxant as Amyl nitite before meals to relax the cardiac sphincter علاج مؤقت -Repeated dilatation of the sphincter • Surgical: Cardiomyotomy operation ( Hiller’s operation) Division of the muscle fiber without injury of the mucosa
شكرا أد مسعد السيسي