Download
1 / 35
450 likes | 828 Views
Diseases of the esophagus. Jakub Szmytkowski Dept. of General and Transplant Surgery Ludwik Rydygier School of Medicine Nicolaus Copernicus University, Bydgoszcz, Poland. Esophagus. a muscular tube through which food passes from the pharynx to the stomach 22-28 cm long

E N D
Diseases of the esophagus Jakub Szmytkowski Dept. of General and Transplant Surgery Ludwik Rydygier School of Medicine Nicolaus Copernicus University, Bydgoszcz, Poland
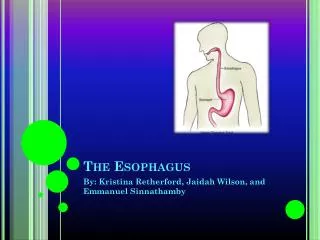
Esophagus • a muscular tube through which food passes from the pharynx to the stomach • 22-28 cmlong • esophagus Latin œsophagus, Greek oisophagos, lit. "entrance for eating."
continuous with the laryngeal part of the pharynx at the level of the C6 vertebra. passes through posterior mediastinum in the thorax and enters abdomen through a hole in the diaphragm at the level of the tenth thoracic vertebrae (T10). divided into cervical, thoracic and abdominal parts due to the inferior pharyngeal constrictor muscle, the entry to the esophagus opens only when swallowing or vomiting Esophagus - anatomy
Esophagus - constrictions • has three anatomic constrictions at the following levels: • At the esophageal inlet, where the pharynx joins the esophagus, behind the cricoid cartilage (14–16 cm from the incisor teeth). • Where its anterior surface is crossed by the aortic arch and the left brocnhus (25–27 cm from the incisor teeth). • Where it pierces the diaphragm (36–38 cm from the incisor teeth).
Esophagus - sphincters • At rest, the esophagus is closed at both ends by the upper esophageal sphincter (UES) at the top, and the lower esophageal sphincter (LES) at the bottom. • LES constricted at all times other than during swallowing and vomiting to prevent the contents of the stomach from entering the esophagus.
Esophagus - histology • mucosa • nonkeratinized stratified squamous epithelium: rapid turnover, protective effect due to the high volume transit of food, saliva and mucus. • lamina propria: sparse. • muscularis mucosae: smooth muscle • submucosa: Contains the mucous secreting glands (esophageal glands), and connective structures (papillae). • muscularis propria : • upper third, or superior part: striated muscle • middle third: smooth + striated • inferior third: predominantly smooth muscles • fibroareolar adventitia • No serosa
Esophagus - pathologies • diverticulae • traction • pushing • achalasia • GERD • Barrett’s esophagus • burns • Esophageal varices • Neoplasms: benign / malignant
an outpouching of the esophageal wall due to traction (inflammatory process) or pulsion Zenker’s diverticulum – border between pahyrynx and esophagus, false symptoms: regurgitation, halitosis, dysphagia, lump on the neck diagnostics: endoscopy, contrast X-ray Esophageal diverticulae
Esophageal diverticulae - treatment • Endoscopic: transection of the septum • Surgical: excision
Achalasia (cardiospasm) • Esophageal motility disorder, cause unknown • Incomplete LES relaxation, increased LES tone, lack of peristalsis • Difficulty swallowing, regurgitation, sometimes chest pain • Treatment: lifestyle changes (careful chewing, water with meals), Ca blockers, botulinum toxin (up to 6 mths), Heller myotomy
usually caused by changes in the barrier between the stomach and the esophagus, including abnormal relaxation of the LES, hiatal hernia chronic symptom of mucosal damage caused by stomach acid coming up from the stomach into the esophagus Symptoms: heartburn, coughing, regurgitation, chest pain Causes: smoking, wrong dietary habits, obesity Treatment: lifestyle changes, PPI’s, H2 blockers Gastro-espohageal reflux (GERD)
Barret’s esophagus • an abnormal change (metaplasia) in the cells of the lower portion of the esophagus. When the normal stratified squamous epithelium lining of the esophagus is replaced by simple columnar epithelium with goblet cells (cells usually found lower in the gastrointestinal tract), Barrett's esophagus is diagnosed. • Associated with esophageal cancer
Esophagitis • Bacterial ,viral, fungal (AIDS, chemotherapy, diabetes, steroid therapy)
Esophageal burns • Acid burns: coagulative necrosis, self – limiting, rarely perforate, often strictures • Base burns: liquefactive necrosis submucosal thrombosis often lead to perforation and mediastinitis • Do not provoke vomiting second exposition • Early endoscopy, do not perform endoscopy betwee 5-15 day postburn • Endoscopic treatment of strictures
Espohageal perforation • 56–90% iatrogenic (endoscopy, endoscopic dilation of strictures, nasogastric tube placement, Sengstaken tube, endoscopy for GI bleeding) • upon forceful vomiting and / or cough • Abdominal, thoracic trauma • foreign body ingestion
Spontaneous perforation of the oesophagus due to vomiting in most cases the tear occurs at the left postero-lateral aspect of the distal oesophagus and extends for several centimeters fatal in the absence of therapy Mackler's triad which includes chest pain, vomiting and subcutaneous emphysema, while classical, is only present in 14% pleural effusion (80%) pain can occasionally radiate to the left shoulder Hamman's sign - a crunching, rasping sound, synchronous with the heartbeat, heard over the precordium in spontaneous mediastinal emphysema produced by the heart beating against air-filled tissues Boerhaave syndrome
Esophageal rupture - treatment • Broad – spectrum antibiotics • Surgical repair • Anti – shock therapy • Chest / mediastinum drainage • Nil by mouth, TPN • Mortality despite treatment 25%
Mallory – Weiss syndrome • Longitudinal tear of mucous membrane • Most frequently due to vomiting • Treatment: endoscopy
Esophageal varices • extremely dilated sub-mucosal veins in the lower third of the esophagus • most often a consequence of portal hypertension, commonly due to cirrhosis; patients with esophageal varices have a strong tendency to develop bleeding • Diagnosis: endoscopy • Treatment: endoscopic banding, surgery • Haemorrhage, if endoscopy unavailable: Sengstaken tube
Esophagus - neoplasms • Benign: myoma, lipoma, fibroma, hemangioma • Malignant: squamous cell cancer, adenocarcinoma • Third most frequent malignancy of the GI tract • Most of the people diagnosed with esophageal cancer have late-stage disease, because symptoms usually do not appear until half of the lumen is obstructed, by which point the tumor is fairly large
Esophageal cancer –palliative treatment • Dilation • Brachyterapy • Laser therapy • Endoscopic stenting