Download
1 / 22
220 likes | 315 Views
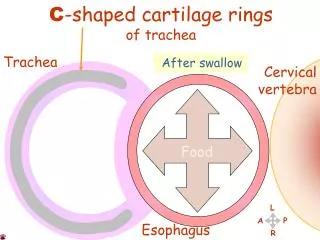
Disease of Esophagus. Gastro- oesophageal reflux disease. Gastro-oesophageal reflux resulting in heartburn affects approximately 30% of the general population. Pathophysiology.

E N D
Gastro-oesophageal reflux disease • Gastro-oesophageal reflux resulting in heartburn affects approximately 30% of the general population
Pathophysiology • Occasional episodes of gastro-oesophageal reflux are common in health. Reflux is normally followed by oesophageal peristaltic waves which efficiently clear it, alkaline saliva neutralises residual acid, and symptoms do not occur. Gastro-oesophageal reflux disease develops when the oesophageal mucosa is exposed to gastroduodenal contents for prolonged periods of time, resulting in symptoms and, in a proportion of cases, oesophagitis.
Hiatus hernia • Herniation of the stomach through the diaphragm into the chest. • causes reflux because the pressure gradient between the abdominal and thoracic cavities, which normally pinches the hiatus, is lost. In addition, the oblique angle between the cardia and oesophagus disappears. Many patients who have large hiatus hernias develop reflux symptoms, but the relationship between the presence of a hernia and symptoms is poor. Hiatus hernia is very common in individuals who have no symptoms, and some symptomatic patients have only a very small or no hernia. Nevertheless, almost all patients who develop oesophagitis , Barrett's oesophagus or peptic strictures have a hiatus hernia.
Clinical features • The major symptoms are heartburn and regurgitation, often provoked by bending, straining or lying down. 'Waterbrash', which is salivation due to reflex salivary gland stimulation as acid enters the gullet, is often present. The patient is often overweight. Some patients are woken at night by choking as refluxed fluid irritates the larynx. Others develop odynophagia or dysphagia. A variety of 'extra-oesophageal' features have been described such as atypical chest pain which may be severe, can mimic angina and may be due to reflux-induced oesophageal spasm. Others include so-called 'acid laryngitis', recurrent chest infections, chronic cough and asthma . The true relationship of these to gastro-oesophageal reflux disease remains unclear.
There is a poor correlation between symptoms and histological and endoscopic findings.
2. Barrett's oesophagus • is a pre-malignant condition in which the normal squamous lining of the lower oesophagus is replaced by columnar mucosa containing areas of intestinal metaplasia. It occurs as an adaptive response to chronic gastro-oesophageal reflux and is found in 10% of patients undergoing gastroscopy for reflux symptoms.
Barrett’s oesophagus. Tongues of pink columnar mucosa are seen extending upwards above the oesophago-gastric junction.
The epidemiology and aetiology of columnar lined oesophagus (CLO) are poorly understood. The prevalence is increasing, and it is more common in men (especially white) and those over 50 years of age. It is weakly associated with smoking but not alcohol. Cancer risk is more closely related to the severity and duration of reflux rather than the presence of CLO per se and It has been suggested that duodenogastro-oesophageal reflux containing bile, pancreatic enzymes and pepsin in addition to acid may be important in pathogenesis.
Diagnosis of Barrett's The molecular events underlying progression of CLO to dysplasia and cancer are incompletely understood but inactivation of the tumour suppression protein p16 by loss of heterozygosity or promoter hypermethylation is a key event, followed by somatic inactivation of p53 which promotes aneuploidy and tumour progression. • This requires multiple systematic biopsies to maximise the chance of detecting intestinal metaplasia and/or dysplasia.
Management of Barrett's • Neither potent acid suppression nor anti-reflux surgery will stop progression or induce regression of CLO. • Regular endoscopic surveillance can detect dysplasia and malignancy at an early stage and may improve survival.
About the Surveillance • Patient without dysplasia should undergo endoscopy every 2-3 years • Those with low-grade dysplasia at 6-12-monthly intervals. • Oesophagectomy is widely recommended for those with high-grade dysplasia (HGD) or intramucosal carcinoma .
3. Anaemia • Iron deficiency anaemia occurs as a consequence of chronic, insidious blood loss from long-standing oesophagitis.
4. Benign oesophageal stricture • Fibrous strictures develop as a consequence of long-standing oesophagitis. Most patients are elderly and have poor oesophageal peristaltic activity. They present with dysphagia which is worse for solids than for liquids. • Diagnosis is by endoscopy, when biopsies of the stricture can be taken to exclude malignancy. Endoscopic balloon dilatation is helpful. • Subsequently, long-term therapy with a PPI drug at full dose should be started to reduce the risk of recurrent oesophagitis and stricture formation. The patient should be advised to chew food thoroughly.
Investigations • Young patients who present with typical symptoms of gastro-oesophageal reflux, without worrying features such as dysphagia, weight loss or anaemia, can be treated empirically without investigation. • Investigation is advisable if patients present in middle or late age, if symptoms are atypical or if a complication is suspected. Endoscopy is the investigation of choice. • Twenty-four-hour pH monitoring is indicated if the diagnosis is unclear or surgical intervention is under consideration.
Management of Gastro-oesophagealreflux disease • Lifestyle advice, including weight loss, avoidance of dietary items which the patient finds worsen symptoms, elevation of the bed head in those who experience nocturnal symptoms, avoidance of late meals and giving up smoking, are recommended. PPIs are the treatment of choice. Symptoms usually resolve and oesophagitis heals in the majority of patients. Recurrence of symptoms is common when therapy is stopped and some patients require life-long treatment at the lowest acceptable dose. • When dysmotility features are prominent, domperidone can be helpful. • There is no evidence that H. pylori eradication has any therapeutic value. • Patients who fail to respond to medical therapy, those who are unwilling to take long-term PPIs and those whose major symptom is severe regurgitation should be considered for laparoscopic anti-reflux surgery.
Other causes of oesophagitis • Oesophageal candidiasis occurs in debilitated patients and those taking broad-spectrum antibiotics or cytotoxic drugs. It is a particular problem in AIDS patients, who are also susceptible to a spectrum of other oesophageal infections • Corrosives: Suicide attempt by strong household bleach or battery acid • Drug: Potassium supplements, NSAIDs, Bisphosphonates, especially alendronate • Eosinophilicoesophagitis.