Download
1 / 45
500 likes | 633 Views
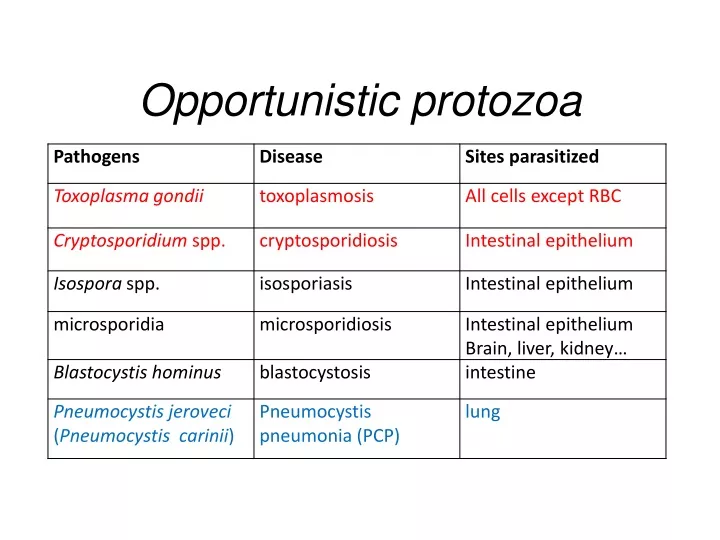
Opportunistic protozoa. Toxoplasma gondii (toxoplasmosis). Introduction. Toxoplasma gondii has very low host specificity, and it will probably infect almost any mammal. It invades all kinds of cells except RBC

E N D
Introduction • Toxoplasma gondii has very low host specificity, and it will probably infect almost any mammal. It invades all kinds of cells except RBC • Cats (both domestic and wild) are the only definitive hostsand can also be the intermediate hosts • The disease that Toxoplasma gondii caused (toxoplasmosis) has been found in virtually every country of the world • Toxoplasmosis is a significant cause of morbidity and mortality in AIDS patientsand congenitally infected infants-- opportunistic infection for human
Morphology • Trophozoite • The intracellular parasites (tachyzoite速殖子) are 3x6µm, crescent shaped organisms that are enclosed in a cell membrane to form a pseudocyst (假包囊) measuring 10-100 µm in size
Morphology • Pseudocyst -- intracellular tachyzoites of Toxoplasma gondii
Morphology • A cyst (包囊)of Toxoplasma gondii filled with bradyzoites; cyst in cardiac muscle
Morphology • A sporulated oocyst(卵囊)of Toxoplasma gondii. • The oocyst contains two sporocysts(孢子囊), each of which contain four crescent-shaped sporozoites(子孢子) • Onlycatsproduce and pass Toxoplasma oocysts; approximate diameter = 10 µm
Life Cycle • Two host pattern with alternation of generations----mammal mammal • Toxoplasma gondii is a serious zoonotic parasite that has almost all the warm blooded animals as the reservior hosts (intermediate hosts) • Life cycle includes two phases called the intestinal (or enteroepithelial) and extraintestinal phases
Life Cycle • The intestinal phase occurs in cats only and produces "oocysts" (___ hosts) • Schizogony –schizontmerozoiteasexual reproduction • Gametogony – male & female gamete fertilize oocyst sexual reproduction • Sporogony – sporocyst sporozoites asexual reproduction • The extraintestinal phase occurs in all infected animals (including cats) and produces trophozoites -- asexual reproduction(__ hosts) • Tachyzoites – pseudocysts • Bradyzoites -- cysts
Life Cycle • Toxoplasmosis can be transmitted by ingestion of oocysts (in cat feces) or “pseudocysts" or “cysts"(in raw or undercooked meat) • Shedding of oocysts in faeces is most common in kittens, but can occur in any age of cat • Oocysts can remain infectious for several months and are quite resistant to disinfectants, drying and freezing. Tissue cysts are less resistant, and are destroyed by proper cooking of food
Pathogenesis In general, most of the human population infected with Toxoplasma are asymptomatic carriers There are a number of factors which determine whether an infected host will express disease symptoms The strain of the pathogen (RH strain) The susceptibility of the host -- immunocompromised Age of the host – new born infants Degree of acquired immunity
Pathogenesis The tachyzoites directly destroy host cells
Clinical features • Although Toxoplasma infection is common (~13% overall world prevalence), it rarely produces symptoms in normal individuals • Could be classified as • Congenital toxoplasmosis • Acquired toxoplasmosis
Congenital Toxoplasmosis • Two types: • Asymptomatic Congenital Toxo • 60% of infected • may suffer from Long Term Sequela • Symptomatic Congenital Toxo • 40% of infected • more likely if mother infected in 1st/2nd Trimester • Severe damage to fetus = stillbirth or abortion • or may be severely affected
Asymptomatic Congenital Toxo • Diagnosis: • + IgM titer in serum of newborn (TORCH +) • no overt clinical disease at birth • Long Term Sequela: • within 7 years of birth - children born to women with high levels of Toxo antibodyhad • 2x > frequency of deafness • 60% more microcephaly (small head) • 30% more Low IQ babies
Symptomatic Congenital Toxo • Spontaneous abortion or stillbirths • Bilateral retinochoroiditis (双侧视网膜脉络膜炎) • Microcephalus(小头畸形)or hydrocephalus(脑积水) • Intracerebral calcification(大脑钙化灶) • Neurological Damage • Learning Difficulties • Jaundice(黄疸) and hepatosplenomegaly
Acquired Toxoplasmosis • usually asymptomatic • majority of population was infected • IgG titer is demonstrable for 10 yr. post-infection • Symptoms – flu-like • swollen neck (cervical lymphadenopathy) • fever, malaise(不舒服) • enlarged liver/spleen (hepatosplenomegaly) • mimics infectious mononucleosis(单核细胞增多症)
Toxoplasmosis in AIDS patients • A significant OI(opportunistic Infection in AIDS) • Toxolymphadenopathy(swollen lymph glands) • Toxo encephalitis (TE) & CNS Toxo death • pulmonary Toxo & Toxo pneumonia • UTIs - Toxo urinary tract infections • disseminated Toxo • Peritonitis(腹膜炎), chorioretinitis(脉络视网膜炎), etc.
Immunology • Both humoral and cell mediated immune responses are stimulated in normal individuals • CMI is protective • Th1 cytokines such as IFN-gamma, IL-12 • Humoral response is of diagnostic value
Diagnosis • Microscopic Examination -Smears and Sections • Specimens -Blood, Sputum, CSF, bone marrow -Tissue Biopsy • Animal Inoculation • Serological tests – IHA, IFA, ELISA (IgM/IgG) • PCR & DNA probes
Epidemiology and control • Worldwide cases of congenital toxoplasmosis are estimated at between 140,900 and 1,127,200, based on an estimated rate of 0.1 to 0.8% of 140.9 million live births in 1992 • Some countries have instituted screening programs of pregnant women • About 5-10% of AIDS patients complicated with toxoplasmosis
Reasons of epidemic • Source of oocysts ... • domestic and wild cats, passes tons of oocysts • Persist in environment if moist • reservoir of infective oocysts • Many intermediate hosts with infective stage • reservoir of infective tissue cysts
Epidemiology and control • Transmission route for humans • Infected • by ingestinginfective oocysts(in >4 day old cat feces) • by ingestingtachyzoites or bradyzoitesin rare meat • by receivingbloodor tissueswith “-zoites” • CONGENITALLYby transplacental tachyzoites
Epidemiology and control • Avoid contact with cat feces • Change cat litter daily to prevent infective oocyst formation • Pregnant women should avoid all contact with cats • Instituted screening programmes of pregnant women • Avoid raw or undercooked meat • Handle uncooked meat carefully • Wash your hands
Treatment • Combination Therapy • Pyrimethamine(乙胺嘧啶) plus either • Sulfadiazine(磺胺嘧啶) or • Trisulfapyrimidines(三重磺胺嘧啶) • During pregnancy, • spiramycin(螺旋霉素) until delivery
Summary • Toxoplasma gondii: pathogenesis, clinical features, control • Opportunistic infection • What are the infective stages of toxoplasma gondii? • Please describe the possible consequences of toxoplasma infection in a young lady. • What parasitic diseases can be transmitted by blood transfusion?
Introduction A threat to the quality of surface water and the environment...! • Cryptosporidium is a protozoan parasite in water environment • Have a low infectious dose necessary to infect human as less than 10 organisms • Potentially lethal for immunosuppressed individuals
Introduction • Cryptosporidiosis:an emerging infectious disease • 1907 ---Tyzzer identifies the oocysts of C. muris in mice • 1910 --- Infection is transmitted by oocysts • 1912 --- Description of C. parvum • 1952 --- C. parvum causes morbidity and mortality • 1971 --- Diarrhea in cattle is associated with C. parvum • 1976 --- Human cryptosporidiosis • 1982 --- First case in AIDS patients • 1987 --- first report in Nanjing, China
Introduction • A complex life cycle, with multiple asexual and sexual developmental stages • Causal agent of acute diarrheal disease in human (third major cause of diarrheal disease worldwide) and animals -- zoonosis • Cryptosporidium parvumhas emerged as a very important pathogen worldwide due to its morbidity in AIDS patients • Despite its significance, little is known about this parasite biology and specific chemo- or immunotherapies to treat cryptosporidiosis are yet to be developed
Morphology • Oocysts are spherical to subspherical, measuring from 4-6 m • Acid-fast method:against a blue-green background, the oocysts stand out in a bright red stain • Four banana-shaped red sporozoites and one dark residual body
Clinical features • Latent duration: 1wk -- cryptosporidiosis • immunocompetent patients • acute, self-limiting diarrheal illness (1-2 week duration), and symptoms include • Frequent, watery diarrhea • Nausea • Vomiting • Abdominal cramps • Low-grade fever
Clinical features • immunocompromised persons • Debilitating, cholera-like diarrhea (up to 20 liters/day) • Severe abdominal cramps • Malaise(不适) • Low-grade fever • Weight loss • Anorexia (厌食) • C. parvum infection has also been identified in the biliary tract (causing thickening of the gallbladder wall) and the respiratory system
Diagnosis • Stool examiniation for oocysts • Biopsy of the intestine epithelium • !!Multiple stool samples (at least 3)should be tested before a negative diagnostic interpretation is reported
Diagnosis • Direct fluorescent antibody (FA) assay • ELISA: controls are necessary to determine whether the kit is performing or not • Molecular diagnosis
Epidemiology and control • Transmission is usually fecal-oral, including water-borne and food-borne means • The highly environmentally resistant cyst of C. parvum allows the pathogen to survive various drinking water filtrations and chemical treatments such as chlorination
Epidemiology and control • Swimming pools and water park wave pools have also been associated with outbreaks of cryptosporidiosis • Food can also be a source of transmission, when either an infected person or an asymptomatic carrier contaminates a food supply
Epidemiology and control • Special cautions must be taken by immunocompromised persons : • With HIV/AIDS • Patients receiving treatment for cancer • Recipients of organ or bone marrow transplants • Congenital immunodeficiencies • Avoid: • sexual practicing involving fecal exposure • contacting with infected adults or infected children who wear diapers • contacting with infected animals • drinking or eating contaminated water or food, and exposure to contaminated recreational water • Drink : boiled water; filtered (1um) water or bottled water
Treatment • No safe and effective therapy for cryptosporidial enteritis has been successfully developed • The urgent need of chemotherapy for persons with AIDs has led to administration of a variety of drugs: • Spiramycin (螺旋霉素),Paromomycin (巴龙霉素) • Berberine to contorl diarrhea • All these drugs have met with different levels of success