Download
1 / 24
260 likes | 309 Views
This review discusses epidemiology, colonoscopic features, assessment, management, prognostic factors, and treatment options for rectal neuroendocrine tumors, formerly known as carcinoids.

E N D
Review on Rectal Carcinoid Joint Hospital Surgical Grand Round 15/10/2016
Review on Rectal Neuroendocrine Tumor Joint Hospital Surgical Grand Round 15/10/2016
From “Carcinoid” to “Neuroendocrine Tumors” • 1907 Germany Pathologist Siegfried Oberndorfer • Arises from neuroendocrine cells • “Karzinoid” – “cancerous like” • Neuroendecrine Neoplasm (NEN) • Potential to Metastasize
Epidemiology • Increasing incidence • Quickest rise among all neuro-endocrine neoplasm • Ethnic association in Asian population • Highest incidence • Ito T, Sasano H, Tanaka M, Osamura RY, Sasaki I, Kimura W, et al: Epidemiological study of gastroenteropancreatic tumors in Japan. J Gastroenterol 2010;45:234–243. • Taghavi S, Jayarajan SN, Powers BD, Davey A, Willis AI: Examining rectal carcinoids in the era of screening colonoscopy: a surveillance, epidemiology, and end results analysis. Dis Colon Rectum 2013;56:952–959.
Epidemiology • Xianbin Z, Li Ma2, Haidong B, Jing Z , Zhongyu W, Peng G. Clinical, pathological and prognostic characteristics of gastroenteropancreatic neuroendocrine neoplasms in China: a retrospective study. BMC Endocrine Disorders 2014, 14:54
Epidemiology • Tsai H-J, Wu C-C, Tsai C-R, Lin S-F, Chen L-T, Chang JS (2013) The Epidemiology of Neuroendocrine Tumors in Taiwan: A Nation-Wide Cancer Registry-Based Study. PLoS ONE 8(4): e62487. doi:10.1371/journal.pone.0062487
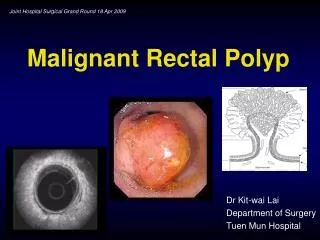
Colonoscopic Features • Small, submucosal tumor • Yellow discolored mucosa • Ulceration, central depression • Located at mid rectum • 75% 5-9.9cm of the anal verge • Kim BN, Sohn DK, Hong CW, Han KS, Chang HJ, Jung KH, et al. Atypical endoscopic features can be associated with metastasis in rectal carcinoid tumors. Surg Endosc. 2008;22:1992---6.
Management – Questions to Answer Assessment Treatment Surveillance
Assessment - Local • Complete colonoscopy • Rectal Ultrasound • Well demarcated, homogenous, isoechoic or hypoechoic lesions • Tumor size and depth • Para-rectal Lymph nodes • Lee SP, Sung IK, Kim JH, Lee SY, Park HS, Shim CS. The effect of preceding biopsy on complete endoscopic resection in rectal carcinoid tumor. J Korean Med Sci. 2014;29:512---8.
Assessment - Systemic • Imaging • Multi-slice contrast CT • MRI • Octreotide scan • PET-scan (Fluorodeoxyglucose, Gallium-68 Dota-octreotide) • Biochemical Markers • Chromagranin A • Role • Detection of metastasis • Local spread and involvement • May not be useful in diagnosis • Staging of High grade / poorly differentiated tumors • Monitoring • Srirajaskanthan R, Kayani I, Quigley AM, Soh J, Caplin ME, Bomanji J: The role of 68 Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111 In-DTPA-octreotide scintigraphy. J Nucl Med 2010;51:875–872. • Gabriel M, Decristoforo C, Kendler D, Dobrozemsky G, Heute D, Uprimny C, et al: 68 Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and CT. J Nucl Med 2007;48:508–518. • Anthony LB, Strosberg JR, Klimstra DS, Maples WJ, O’Dorisio TM, Warner RRP, et al. The NANETS consensus guidelines for the diagnosis and management of gastrointestinal neuroendocrine tumors (nets): well-differentiated nets of the distal colon and rectum. Pancreas. 2010;39:767---74.
Prognostic value - Size • Gleeson F, Levy ML, Dozois EJ, Larson DW, Song L, Boardman LA: Endoscopically identified well-differentiated rectal carcinoid tumors: impact of tumor size on the natural history and outcomes. Gastrointest Endoscopy 2014;80:145–151. • Weinstock B, Ward SC, Harpaz N, Warner RR, Itzkowitz S, Kim MK: Clinical and prognostic features of rectal euroendocrine tumors. Neuroendocrinology 2013; 98: 180–187.
Prognostic value - Size • Fahy BN, Tang LH, Klimstra D et al. Carcinoid of the rectum risk stratification (CaRRs): a strategy for preoperative outcome assessment. AnnSurg Oncol 2007; 14: 1735–1743
Prognostic value - Stage • Gleeson F, Levy ML, Dozois EJ, Larson DW, Song L, Boardman LA: Endoscopically identified well-differentiated rectal carcinoid tumors: impact of tumor size on the natural history and outcomes. Gastrointest Endoscopy 2014;80:145–151. • Weinstock B, Ward SC, Harpaz N, Warner RR, Itzkowitz S, Kim MK: Clinical and prognostic features of rectal euroendocrine tumors. Neuroendocrinology 2013; 98: 180–187.
Treatment >2cm High Risk Metastatic Poor Prognosis <1cm Low Risk 1-2 cm Unclear
Treatment • Low risk • Polypectomy • Endoscopic mucosal resection • EMR based techniques • Cap aspiration • Band snare • Endoscopic submucosal dissection • Transanal endoscopic microsurgery <1cm Options • Angela R, Fernando C, Isabel P: Neuroendocrine Rectal Tumors: Main Features and Management. Portuguese Journal of Gastroenterology. 2.15; 22(5): 213-220 • ENETS Consensus Guideline Update of Colorectal Neuroendocrine Neoplasm (NEN). Neuroendocrinology 2016;103:139–143 • Louis de M, Hedia B, Rodica G, Thierry P, Guillaume C: Updating the management of patients with rectal neuroendocrine tumors. Endoscopy 2013; 45:1039-1046
Treatment • High risk • Same way as adenocarcinoma • Anterior Resection + TME • Abdominal perineal resection Investigations • Systemic Imaging • Biochemical markers >2cm Options • Angela R, Fernando C, Isabel P: Neuroendocrine Rectal Tumors: Main Features and Management. Portuguese Journal of Gastroenterology. 2.15; 22(5): 213-220 • ENETS Consensus Guideline Update of Colorectal Neuroendocrine Neoplasm (NEN). Neuroendocrinology 2016;103:139–143
Treatment: 1-2cm • Yangong H, Shi C, Shahbaz M, Zhengchuan N, Wang J, Liang B, Ruliang F, Gao H, Bo Q, Niu J: Diagnosis and treatment experience of rectal carcinoid (a report of 312 cases). Int J Surg 2014;12:408–411. • Park CH, Cheon JH, Kim JO, Shin JE, Jang BI, Shin SJ, et al. Criteria for decision making after endoscopic resection of well-differentiated rectal carcinoids with regard to potential lymphatic spread. Endoscopy. 2011;43:790---5.
Treatment • Unclear • Muscularis Propria invasion • Lymphovascular involvement • High grade histology Treatment Investigations • Low Risk • Local Resection +/- Salvage • High Risk • Radical surgery • RUS • +/- Systemic workup 1-2cm Risk Factor
Treatment • Biotherapy • Somatostatin Analogues • Interferon • Systemic Chemotherapy • Peptide-receptor Radiotargeted radiotherapy Surgery • Symptomatic control Metastatic Options • ENETS Consensus Guidelines for the Management of Patients with Digestive Neurodendocrine Neoplasms: colorectal neuroendocrine neoplasms. Neuroendocrinology 2012; 95:88-97 • ENETS Consensus Guideline Update of Colorectal Neuroendocrine Neoplasm (NEN). Neuroendocrinology 2016;103:139–143
In Real Life… • Surveillance • Salvage local resection >1cm Incomplete Resection Risk Factor present • Workup • +/- salvage surgery <1cm Incomplete Resection No Risk factor
Surveillance • Duration 10 years • Modality: colonoscopy, RUS, imaging Endoscopy within 1st year No Follow Up Annual Follow Up Endoscopy Q4-6 months x 1 year Annual Follow Up • ENETS Consensus Guidelines for the Management of Patients with Digestive Neurodendocrine Neoplasms: colorectal neuroendocrine neoplasms. Neuroendocrinology 2012; 95:88-97 • ENETS Consensus Guideline Update of Colorectal Neuroendocrine Neoplasm (NEN). Neuroendocrinology 2016;103:139–143
Conclusion • Increasing incidence • Particularly relevant to Asian population • Prognostic factors • Evolving treatment modalities • Controversy exists