Download
1 / 28
450 likes | 1.26k Views
Chronic Fatigue Syndrome. Camille Bowen. Why Chronic Fatigue? Why am I chronically fatigued?. Overview. History Characteristics Diagnosis What it is Tests Treatments Nutritional recommendations What to know/do Conclusion. History – Initial Finding.

E N D
Chronic Fatigue Syndrome Camille Bowen
Overview • History • Characteristics • Diagnosis • What it is • Tests • Treatments • Nutritional recommendations • What to know/do • Conclusion
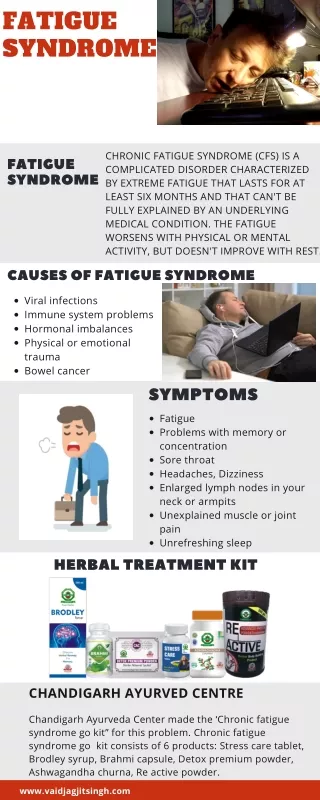
History – Initial Finding • Fatigue with hypothyroidism, chronic heart failure, multiple sclerosis, depression • 1980 -1st recognized as medical condition • Persistent or relapsing fatigue
History- Unknown disease • Many names from speculated cause: • “Post-viral fatigue syndrome” • “Myalgic encephalomyelitis” • “Neuromyasthnia” • 1988 CDC defined it Chronic Fatigue Syndrome (CFS) • Prevalence 0.2-2.6 % • Cause: unknown no treatment • No geographic/ethnic difference • Twice as prevalent in women
Characteristics • Severe and disabling fatigue • Headache (90%) • Difficulty concentrating (90%) • Sore throat (85%) • Tender lymph nodes (80%) • Muscle/joint aches (75%) • Fever (75%) • Difficulty sleeping (70%) • Psychiatric problems (65%) • Rapid pulse (10%)
Current Diagnosis • 1994 CDC published diagnostic criteria for CFS • Sever fatigue for 6 months with • 4 or more physical symptoms • Memory impairment • Tender lymph nodes • Joint pain • Headache • Unrefreshing sleep • Postexertional malaise (>24 h)
Exclusion criteria: • Active, unresolved, suspected disease causing fatigue • Depression (psychotic, melancholic, bipolar) • Psychotic disorders • Dementia • Anorexia/bulimia nervosa • Alcohol/substance misuse • Severe obesity
What is CFS?—hypothesis • Hypothalamo-pituitary-adrenal (HPA) axis—major role in regulating stress response • Stress related disorders, CFS, fibromyalgia, chronic pelvic pain, post traumatic stress disorder alterations in HPA axis • Most studies show underactive HPA • Body’s adaption to chronic stress (Burnout) • Contradictory results
CFS-what it is • No structural problem with endocrine organs= functional • Noted- patients selected for study, methods used for investigation, stage of syndrome when tested, interpretation of the results. • Pathogenesis: unknown; multiple causes studied
CFS-what it is • Chronic stress may switch from hyper- to hyporesponsiveness • Defect at/above level of the hypothalamus, resulting in a deficiency in release of CRF and/or other secretagogues • Level of HPA axis dysfunction correlated to length of illness
CFS- what it is • Corticotropin-releasing factor (CRF) • excitatory peptide and has analgesic properties. Reduced availability = lethargy and pain
CFS-what it is • Main Findings: • Hypocortisolism • Blunted ACTH responses • Enhanced negative glucocorticoid feedback • Still don’t know the cause
CFS • Large longitudinal studies needed to examine how HPA axis disturbances evolve over time and determine if they precede the development of stress-related disorders • difficult because only small percentage of stressed individuals develop CFS symptoms
Tests • Determine HPA axis function through: • Insulin tolerance test (ITT) • Short ACTH (250ug) stimulation test • Low-dose ACTH (1ug) stimulation test • CRH stimulation test • Metyrapone test • Glucagon test • AVP stimulation test
Tests • Example: peak cortisol after ITT <500/550 nmol/l = underactive HPA axis IQ : tests insert substance into body and measure levels (cortison, ATPH,) • Abnormal suggests HPA axis dysfunction • Each test has its limitations (no standardization, chemical availability limited, reproducibility problems)
Treatments • No medical treatments • Some tendency for spontaneous improvement
treatments • Study #1: 136 patients • Physical activity & antidepressant • Physical activity & placebo • Therapist & antidepressant • Therapist and placebo • Physical activity: less fatigued, more fit • Antidepressant: helped depression symptoms
treatments • Study #2: • Aerobic activity OR flexibility & relaxation therapy • Aerobic training = fitness, muscle strength, less fatigue • Flexibility & relaxation= significantly less effect
treatments • Study #3: • Medical care • Face to face- explained symptoms, designed exercise program • Telephone consultation • Face to face consultation • 69% had satisfactory physical functioning • Improved fatigue, mood, sleep, & disability (phys. activity or psychological support) • Other groups—therapy alone doesn’t help patient’s symptoms
TreatmentAcupuncture/Moxibustion • More effective than cortisone • Response rates: 78-100% • Quality of the studies were poor: • Poor design • No standard evaluation • None mentioned blinding clinicians, subject, or raters
Treatments Physical activity— low intensity to moderate; increase duration AND • Cognitive behavioral therapy • Phys. activity increases muscle strength, stamina, endurance = better daily life Chemicals released = better mood, less pain
Treatments • Establish sleep routine—going to bed, wake-time • Schedule activity— be consistent • Switch from “feeling” to “ability” • Adolescents & children: family therapy approach
Nutrition Claims • Probiotics • Antifungal agents • Vitamin/mineral supplementation • Dietary change
Nutrition • One study- improved MRI scans with ultra-pure EPA and n-6 long-chain polyunsaturated fatty acids • Neurocognitive functions improved in pilot study using probiotics • Preliminary glutamine supplementation- improved mood & appetite, decreased muscle pain, increased physical activity.
Nutrition • Low sugar low yeast (LSLY) diet • Study showed very difficult to follow • Healthy eating (HE) diet is more practical • Insures adequate nutrient • Multivitamin supplements • not supported by research • may help in overall improvement of diet
Overall- yes to what? • Basic healthy eating • Probiotics • Possible supplements • Exercise routine • Sleep schedule • Cognitive behavior therapy • More research is needed!
conclusion • History • Characteristics • Diagnosis • Hypothesis/what it is • Tests • Treatments • Nutritional recommendations • Summed up what to do