Download
1 / 72
750 likes | 1.34k Views
Facial Nerve Paralysis. Dr. Vishal Sharma. Gabriel Fallopius (1523-62). Anatomy of Facial Nerve. Motor root: 7000 axons Sensory root (Nervus intermedius / Wrisberg): 3000 axons. Joins motor root at fundus of I.A.C. Motor: predominantly to facial muscles

E N D
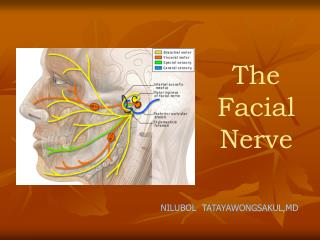
Facial Nerve Paralysis Dr. Vishal Sharma
Anatomy of Facial Nerve • Motor root:7000 axons • Sensory root (Nervus intermedius / Wrisberg): 3000 axons. Joins motor root at fundus of I.A.C. • Motor:predominantly to facial muscles • Secretomotor:lacrimal, submandibular, sublingual • Taste:anterior 2/3rd of tongue • Sensory:Post-aural / concha / ext. auditory canal
Parts of facial nerve Intracranial: within cerebello-pontine angle Intra-temporal Meatal segment Labyrinthine segment Tympanic segment Mastoid segment Extra-cranial Extra-parotid Intra-parotid (terminal)
Segments of Facial Nerve 1. Supranuclear:Fibers in cerebral cortex to brain stem 2. Brain stem:Motor nucleus of facial nerve (pons) 3. Intra-cranial (12 mm): Brain stem to entry into IAC 4. Meatal (10 mm):Within Internal Auditory Canal 5. Labyrinthine (4 mm):Fundus of I.A.C. to Geniculate gangl. 6. Tympanic (11 mm):Geniculate ganglion to pyramid 7. Mastoid (13 mm):Pyramid to stylomastoid foramen 8. Extra-temporal (15 mm):S.M. foramen to pes anserinus
Primary branches of facial nerve Intra-temporal: greater superficial petrosal, stapedius, chorda tympani Extra-parotid:post-auricular, stylohyoid, posterior belly of digastric Intra-parotid: temporal, zygomatic, buccal, marginal mandibular, descending cervical
Communicating branches to: Meatal: vestibulo-cochlear Tympanic: lesser petrosal otic ganglion Mastoid: auricular branch of vagus Extra-parotid: glossopharyngeal, auriculotemporal, vagus, greater auricular, lesser occipital Terminal: branches of trigeminal
Cochleariform process:small bony protuberance (from which tensor tympani muscle turns 900 to insert into malleus) lies 1 mm inferior to geniculate ganglion at anterior end of tympanic segment. Cog: bony ridge hanging from tegmen tympani lies 1 mm above & posterior to cochleariform process. Incusshort process:2 mm below lies external genu Lateral Semicircular Canal: 2 mm Antero-Infero-Medial lies external genu Oval window:1 mm above lies external genu
Inferior edge of Posterior S.C.C.:2 mm anterior & lateral lies mastoid segment of facial nerve Tympano-mastoid suture in posterior canal wall:5-8 mm medial lies mastoid segment of facial nerve Digastric ridge in mastoid tip:leads antero-medially to mastoid segment of facial nerve Groove between mastoid & bony E.A.C. meatus: bisected by facial nerve Tragal pointer:1 cm antero-infero-medial is facial nv Root of styloid process: lateral lies facial nerve Superior border of posterior belly of digastric: superior & parallel lies facial nerve
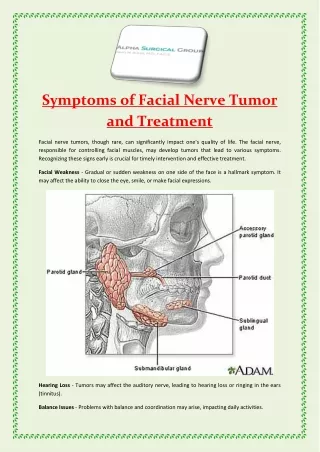
1. Idiopathic (55%):Bell’s palsy, Melkersson Rosenthal syndrome 2. Temporal bone trauma (25%): Road traffic accident 3. Infection (10%):C.S.O.M., Herpes Zoster oticus Malignant otitis externa 4. Neoplasm (5%): Parotid tumors, Acoustic Neuroma, Glomus tumors, Malignancy of ear 5. Congenital (4%):Moebius syndrome 6. Iatrogenic (rare): Mastoidectomy, Parotid surgery 7. Metabolic (rare):Diabetes mellitus, Hypertension
Diagnosis • Topo-diagnostic Tests • Electrical Tests • Magnetic stimulation of intra-cranial facial nerve • CT scan temporal bone: for progressive palsy • MRI brain • Surgical exploration
Topo-diagnostic tests • Audiometry:cochlear nerve function • Vestibulometry:vestibular function • Schirmer’s test:Greater Superficial Petrosal Nerve • Stapedial reflex test: Nerve to stapedius • Electrogustometry:Chorda tympani • Submandibular salivary flow: Chorda tympani • Examination for terminal facial nerve branches
Schirmer’s Test Unilateral wetness ed by >30% of total amount of both eyes after 5 minutes = Schirmer test positive lesion at or proximal to geniculate ganglion
Electrogustometry Measures minimum amount of current required to excite sensation of taste
Nerve Excitability Test • Stimulating electrode used over terminal branches of facial nerve • Minimum current intensity required to produce minimal muscle movement is calculated • Normal side compared to paralyzed side • Difference > 3.5 mAmp = unfavorable prognosis
Maximal stimulation test • Stimulating electrode used over terminal branches of facial nerve • Minimum current intensity required to produce maximal muscle movement is calculated • Normal side compared to paralyzed side • Difference > 3.5 mAmp = unfavorable prognosis
Electro-neuronography • Terminal branch of facial nervestimulated & action potential recorded in appropriate muscle • Paralyzed side compared to normal side (which is taken as 100%) • Response > 10% = 85-95 % chance of recovery • Response < 10% = 25 % chance of recovery
Electromyography Records spontaneous activity of facial muscles
Electromyography Responses Normal Polyphasic Fibrillation Electrical Silence