Download
1 / 16
190 likes | 498 Views
Working with Communication and Swallowing Problems. Sarah Maslin Sarah Holdsworth Speech and Language Therapists Therapy assistant Conference November/December 2013. Aims and Objectives. To outline the role of the Speech and Language Therapist (SLT) in a range of settings

E N D
Working with Communication and Swallowing Problems Sarah Maslin Sarah Holdsworth Speech and Language Therapists Therapy assistant Conference November/December 2013
Aims and Objectives • To outline the role of the Speech and Language Therapist (SLT) in a range of settings • To discuss communication and swallowing problems • To think about how you as Therapy Assistants can help when working with these patients
Myths and TruthsTrue or False? • Everyone with a swallowing problem should have thickener in their drinks • Only Doctors/nurses can refer to SLT • If someone can’t speak they won’t understand what I am saying • SLT can advise around communication support strategies (visual charts, gesture)for patients • Patients having difficulty with medication, The SLT needs to assess their swallowing.
What do we do? Communication Swallowing
What can cause some of these problems? • CVA • Parkinson’s Disease • Motor Neurone Disease • Multiple Sclerosis • Huntingdon’s Chorea • Myasthenia Gravis • Head Injury • Brain Tumour • Dementia • Head and neck cancer • Tracheostomy/intubation • Developmental / congenital conditions
Types of Communication Problems • Dysphasia (or aphasia): difficulty understanding or producing language (words, sentences, conversation), which may include reading and writing • Dysarthria difficulty producing clear speech, “slurred” speech, due to muscle weakness • Dyspraxia difficulty planning how to pronounce words (can also affect planning other types of movements) • Dysfluency stammering / stuttering Types of Communication Problems • Dysphonia difficulty producing adequate voice, from hoarse voice to total loss of voice
What do SLTs do with communication impairments? • Assess and diagnose communication impairments • Direct work with clients • Work with communication partners • Compensatory strategies • Support or confidence building in specific situations • Communication support for specific discussions or decision making
Communication Tips • Glasses and hearing aids • Give your full attention • Sit or stand at the same level as the person • Give eye contact • Speak slowly and use simple language • Ask yes/ no questions • Give additional time for communication • Reduce distractions and background noise as possible • Make use of gestures, facial expression, writing and pictures to support your communication • Understand the specific difficulty – speak to the SLT
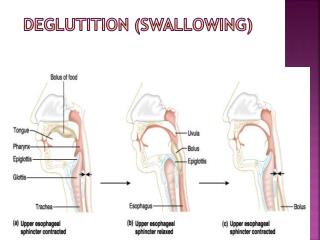
Swallowing Problems with swallowing known as“dysphagia”
Definitions What do you understand by the term? • Aspiration • Aspiration pneumonia • Feeding at Risk
Signs and symptoms of a swallowing problem • Coughing whilst eating and drinking • A ‘wet’ or gurgly voice after swallowing • Shortness of breath after eating and drinking • Choking, red face and watering eyes • Food or drink coming down the nose • Pain or discomfort on swallowing • Difficulties chewing • Excessive drooling • Difficulties clearing the mouth of all food after a meal
How do we manage swallowing problems • Bedside assessment • Therapy • Diet or fluid texture modification • Specific postures/ manoeuvres • Training • Objective assessment • Non-oral nutrition/ hydration
Case study 1 • John, aged 70, in hospital following CVA • Expressive and receptive dysphasia • John can produce single words if given time to respond and he often makes mistakes e.g. says “bath” when means “bed” • SLT have provided a communication chart – John can correctly point to pictures of what he wants / needs • Can understand simple phrases but not long complex sentences • Think about how you would facilitate this patients communication in one of your sessions?
Case study 2 • Claire, 40 Attending MDH for OT and Physio, • Recently discharged from hospital following CVA • Patient complaining of poor saliva management and you notice when drinking in sessions patient clearing her throat. • Patient feels generally well in herself • How would you manage this?