Download
1 / 29
300 likes | 451 Views
Advances in the Management of BPH. Mr C Dawson Consultant Urologist Edith Cavell Hospital Peterborough. Advances in the Management of BPH. Mr C Dawson Consultant Urologist Fitzwilliam Hospital Peterborough. The Scale of the Problem.

E N D
Advances in the Management of BPH Mr C Dawson Consultant Urologist Edith Cavell Hospital Peterborough
Advances in the Management of BPH Mr C Dawson Consultant Urologist Fitzwilliam Hospital Peterborough
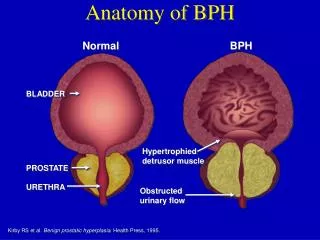
The Scale of the Problem • Moderate to severe Lower Urinary Tract Symptoms (LUTS) occur in 25% of men over 50 years, and the incidence rises with age • Approximately 90% of men will develop histological evidence of BPH by 80 years of age
The Scale of the Problem Increasing because: • Men are living longer • Proportion of Men over 50 years will increase • Men are better informed about health matters
Difficulties in Diagnosis and Management • The symptoms of BPH are the same as those of early Prostate Cancer • Confirmation of the presence of prostate cancer may be difficult • The need to treat (proven) cancer may not always be clear cut
Storage Symptoms Frequency Nocturia Urgency Urge incontinence Bladder Pain Understanding Lower Urinary Tract Symptoms (after Abrams, Bristol, UK) • Voiding Symptoms • Slow stream • Intermittent flow • Hesitancy • Straining • Terminal dribble
Physical Signs • May be few • Look for obvious uraemia • Palpate for full bladder • Examine urethral meatus and palpate urethra for stricture • DIGITAL RECTAL EXAMINATION (DRE) !!
Investigations for BPH • Urea and electrolytes if clinically indicated • PSA (should we counsel patients?) • Ultrasound urogram • Flow rate (if you have access) • IPSS
A word about Prostate Cancer • No symptoms specificfor early prostate cancer • Presenting symptoms are therefore those of BPH • Biopsy of the prostate should be performed in those with abnormal DRE, or PSA above age-specific reference range
Prostate Specific Antigen • Single-chain glycoprotein of 240 aa residues and 4 carbohydrate side chains • Physiological role in lysis of seminal coagulum • Prostate specific, but NOT cancer specific
Prostate Specific Antigen In addition to prostate cancer, an elevated level may be found in • Increasing age • Acute urinary retention / Catheterisation • after TURP / Prostate Biopsy • Prostatitis • BPH A reduced level may be found in patients treated with Finasteride
The Problem with PSA • Men with Prostate Cancer may have a normal PSA • Men with BPH or other benign conditions may have a raised PSA • May not even be prostate-specific! • What to do with men with a PSA of 4-10 ng/ml PSA = Persistent Source of Anxiety?
Refinements in the use of PSA • PSA density • PSA Velocity • Age-Specific PSA 40-49 Years old <2.5ng/ml 50-59 Years old <3.5ng/ml 60-69 Years old <4.5ng/ml 70-79 Years old <6.5ng/ml • Free:Total PSA ratio (<0.15 strongly suggests possibility of Ca Prostate)
Prostate Specific Antigen Possibly Some Attributes
The Management of BPH • Advances in the Management of BPH
New treatment modalities for BPH • -blocker therapy (including selective blockers of -1a receptors) • 5- -reductase inhibitors - Finasteride (Proscar) • Minimally invasive Techniques • Transurethral Microwave Thermotherapy (TUMT) • Transurethral Needle ablation (TUNA) • Transrectal high-intensity focused ultrasound (HiFU) • Transurethral electrovaporisation (TUVP)
Pharmacotherapy for BPH • Alpha-blockers remain an important therapy • Selective -1a receptor blockers may have fewer side effects
Pharmacotherapy for BPH • Finasteride (Proscar) - PLESS study has confirmed that men with large prostates (>40cc), taking long-term therapy, less likely to develop acute retention, or require surgical intervention
Minimally invasive therapies • High energy TUMT, and TUNA, have proven clinical efficacy between that of drug therapy and TUVP or laser therapy • HiFU currently requires GA, is costly and time consuming, and appears unlikely to be popular at present • The subjective response after MITs and TURP appear similar, but objective results superior for TURP
Surgical Therapies • TURP still the gold standard therapy, with which all other therapies must be considered • Laser therapy • expensive to set up • Significantly reduced blood loss • Catheter may be required post operatively • Open Prostatectomy rarely required
ECH Urology Department Guidelines for the Management of BPH • Produced after discussion between working party of General Practitioners and Consultants • Agreed within the department of Urology
Future perspectives for the management of BPH • Much more emphasis on Quality of Life • Minimally invasive therapies are improving and may yet challenge the superiority of TURP
Conclusions - BPH • Remains an important cause of patient morbidity • Correct approach to assessment is important • Many men may have their symptoms relieved by alpha blocker therapy or Finasteride, which has also been shown to reduce the likelihood of surgery or acute urine retention
Conclusions - BPH • A large variety of MITs exist for BPH who fail drug therapy, but for most patients the gold standard surgical procedure remains TURP • The next few years will see many more techniques available to challenge the position of TURP