Download
1 / 106
1.11k likes | 1.48k Views
BPH MANAGEMENT. MINIMALLY INVASIVE AND ENDOSCOPIC TECHNIQUES. BPH Minimally Invasive Rx Options. Urethral stents TUNA Microwave thermotherapy- TUMT Laser Therapy Hydrothermotherapy. Indications for Invasive Therapy for BPH. Failure of medical therapy Urinary retention->1/3 bladder vol.

E N D
BPHMANAGEMENT MINIMALLY INVASIVE AND ENDOSCOPIC TECHNIQUES
BPH Minimally Invasive Rx Options • Urethral stents • TUNA • Microwave thermotherapy- TUMT • Laser Therapy • Hydrothermotherapy
Indications for Invasive Therapy for BPH • Failure of medical therapy • Urinary retention->1/3 bladder vol. • Recurrent urinary infection • Vesicolithiasis • Recurrent hematuria- gross • Azotemia
Criteria for Utilization of Alternative Minimally Invasive Therapies • Less adverse side-effects • Approaches or = surgical outcomes • No Anesthesia • Shorter Hospital stay • Less expensive • Safety profile = /> surgical therapy
Advantages Less adverse effects No anesthesia No hospital stay Cheaper Approaches outcomes of surgery Disadvantages Less favorable outcome, flow & sx’s Retreatment Cost $ & suffering of retreatment Complications- hematuria, dysuria, retention Treatment Options- Minimally Invasive Therapies
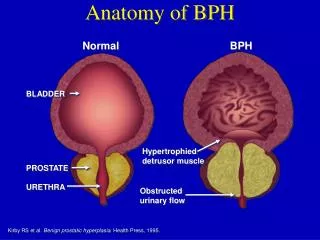
Urethral Stents • Initially conceived to relieve BOO 2º to BPH *, later to urethral stricture • Types- 1. Temporary 2. Permanent • Endoscopic insertion • Major role in patients unfit for surgery *Fabian,1980
Urethral Stent- Temporary • Nonabsorbable removed or changed q6-36 mos. topical with sedation success 50-90% no catheter or cysto with stent in situ complications-encrustation,migration, breakage,stress incont. UTI, hematuria
Urethral Stent-Temporary • Intraurethral Catheter(polyurethrane) • de Pezzer proximal end(like a malecot) • may used after TUMT • 16 Fr,variable to single lengths • Nissenkorn, Barnes, Trestle(two components) • Usually left for 1 month • Complications- hematuria, urinary retention, • Await large multicenter RCT
Urethral Stent- Biodegradable • Polyglycolic acid reinforced • Placed after laser prostatectomy,TUMT • Voiding difficulty at 3-4 wks, transient • Cost-effectiveness questioned,added to TULP or TUMT • Await long term, multi-center RCT
Urethral Stent-Permanent • Attempt to permanently, definitively treat BOO 2º BPH • Initial enthusiasm turned to present literature silence • Initially introduced to Rx USD • Present use-USD,S-D dyssyner., post- brachytherapy,
Urethral Stent- Urolume • Manufactured by AMS, for BPH patients • Modified both stent and delivery device • Lengths vary from 1.5 –4.0 cm • Symptoms scores improve 8-9 pts. • Flow rates improve 4-6cc/sec(peak) • Used in nonsurgical candidates • Interest has waned with Tuna and TUMT
Urethral Stent- Urolume • Complications epithelial hyperplasia migration of stent irritative voiding painful ejaculation
Urethral Stent- Others • Memotherm- variable results • ASI –withdrawn from production • Ultraflex-43 fr, 2-6cm, nickel-titanium alloy, used in BPH, D-S dysyner., epithelial hypperplasia and migration low • Conclusion- temporary stents are attractive after TUNA and TUMT
Transurethral Needle Ablation of the Prostate • Heat delivery system to induce necrosis of the prostate tissue to relieve BOO 2º BPH • Aim to prostate temp >60º C • Uses low-level radio frequency energy delivered by needles into prostate • Use of topical anesthesia adequate
TUNA- Delivery of RF Energy • Produced by Vidamed, uses applicator with two needles • Generator produces monopolar RF signal of 490kHz to give excellent tissue penetration • Grounding pad over sacrum large size • Size of prostate lesion f: kHz,time,depth and position of needle insertion
TUNA- Energy Characteristics • RF produces molecular agitation generated heat • Heat generated p: 1/radius • Heat lost by convection, vascularity affects lesion size as RF has no effect on vessels > 2-3mm diameter • RF hotter central area and quick decline of temp as distance from needles 4
TUNA- Experimental Data • TUNA creates 1cm necrotic lesion with no damage to rectum, bladder base, or distal prostatic urethra • Necrosis maximal @ 7 days, fibrosis by 15 days • Treated areas have absence of staining of PSA,smooth mus. actin, -adrenergic nerual tissue(maximal @ 1-2 weeks)
TUNA-Experimental Data • Sequential injury to different types of nerve endings may occur NOS* most vulnerable • Central core Temp- 90-100ºC, edge of zone 50ºC • Treatment times of 5-7 min. needed to produce coagulation necrosis in Rx Site *NOS- nitric oxide synthase
TUNA-Instruments RF needles deployed Note insulation and bare tips
TUNA-Treatment • Position- dorsolithotomy • Anesthesia-local, sedation, SAB, Gen • Instrument/needle placed with 0º telescope • Needle deployed/activated-20x10mm lesion • Two lesions/needle deployment-1 pair/3cm, 2 pair/4cm, additional pair/cm urethral length; Rx bilaterally • RF power delivered @2-15W for 5min., catheter is optional
TUNA-Summary of Data for 546 Patients* Summary of world experience @12 months follow-up
TUNA- Adverse Effects • Urinary retention-13-42% • Irritative voiding-40% (1-7days) • UTI-3% • Urethral stricture-1.5% • Hematuria-33%, mild, short-lived • Reoperation-12-14% in 2 yrs
TUNA-Indications • BPH/BOO • Lateral lobe enlargement • Prostate volume <60gms • Median lobe not ideal, but can be Rx • Bladder neck hypertrophy not ideal candidate
TUMT-Transurethral Microwave Therapy • Evaluated for past decade • Widely used, variable urologist attitude • Evolution from low-energy to high-energy • Presently most commonly used devices are Prostatron and Targis • Current methods use either urethral cooling catheter or non-cooling catheter
TUMT- Method of Action • Heat induced hemorrhagic necrosis, sympathetic nerve injury, apoptosis • Tissue exposed to 45ºC for 60 min suffered hemorrhagic necrosis • Sympathetic nerve injury histologically confirmed in 2 reports… • Suggests thermal injury to adrenergic fibers likely accounts for symptoms
TUMT-Method of Action • Targis antenna(902-1928MHz) exceeds Prostatron(1296MHz) in efficiency of delivery of thermal energy • 1-adrenoreceptor density after TUMT • Adrenergic nerve fibers remain in lamina propria and epithelial layers, virtually absent in smooth muscle layers
TUMT- Method of Action • Apoptosis induced by moderate thermal energy for longer period of time • Hemorrhagic necrosis induced by higher thermal energy over shorter time • Brehmer and Svennson demonstrated poptosis in 76% of cultured prostate cells 24 hrs after heat exposure, only 14% were necrotic
5mm-62.4ºC 10mm-50.5ºC 15mm-temp =urethral Larson and Collins, 1995
TUMT- Clinical Results Three months duration- TUMT vs Sham Blute et al 1996,
TUMT- Clinical Results Six Months Duration- TUMT vs Sham Larson et al 1998
TUMT- Clinical Results Twelve Months Duration- Prostatron 2.5 vs Turp D’Ancona et al 1999, @ 24 mos 8/31TUMT & 1/21 needed other Rx