Download
1 / 36
470 likes | 778 Views
REGULATION of RESPIRATION. Dr.M.B.Bhat. Control of breathing[regulation]. Can be classified into – Central control of breathing – by the neurons (centers) present in the brain –again divided into Voluntary central control & Involuntary or autonomic central control

E N D
REGULATION of RESPIRATION Dr.M.B.Bhat.
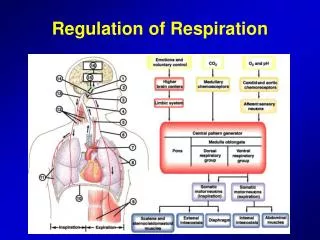
Control of breathing[regulation] • Can be classified into – • Central control of breathing – by the neurons (centers) present in the brain –again divided into Voluntary central control & Involuntary or autonomic central control • Peripheral control of breathing – Control of breathing by nervous (reflexes) & chemical mechanisms
Central control of breathing • Voluntary control system – Center –Neocortex through motor cortex – Efferent through Corticospinal tract – to respiratory motor neurons of the spinal cord • Involuntary control system – Center – Respiratory centers located in Pons & Medulla Efferent to spinal respiratory motor neurons lie between lateral & ventral corticospinal tracts
By both the central control mechanisms -- When motor neurons supplying inspiratory muscles are active, the motor neurons supplying expiratory muscles are inhibited & Vice versa This is done by – Descending pathways which excite agonist muscles inhibit antagonist muscles Reciprocal innervation property of the spinal reflexes
Respiratory centers • Two types • Medullary respiratory centers –contain the main components of the ‘respiratory control generator’ of autonomic respiration • Pontine respiratory centers – control the autonomic respiration by influencing the medullary centers activity.
Medullary Respiratory centers • Two groups of respiratory neurons • Dorsal respiratory group ofneurons • or (DRG neurons) or (Inspiratory) neurons • Ventral respiratory groupof neurons • (VRG neurons) or • E (expiratory) neurons
Dorsal group neurons (DRG) or Inspiratory neurons • Located in & near Nucleus Tractus Solitarius (NTS) • DRG –produce inspiratory ‘Ramp signal’ –Efferent -- from these neurons –project monosynaptically to phrenic motor neurons & motor neurons supply external inter-costal muscles • -- Also to VRG & Apneustic center of pons & stimulate them • Afferent –receive from peripheral chemoreceptors
Ramp signal • Produced by DRG (Dorsal respiratory group neurons) • The impulses (depolarization) generate here weakly first & increases steadily in a ramp fashion for about 2 seconds. Abruptly ceases for 3 seconds & then the cycle repeats again & again • Significance –there is a steady increase in lung volume (rather than inspiratory gasps). • Initiated by “pre-BÖtzinger complex” (recent concept) [Old concept DRG has spontaneous discharge) • Controlled by the factors that regulate respiratory rate by controlling the limiting point at which ramp signal suddenly ceases.
Pre-BÖtzinger complex (pre-BÖTC) • It has got ‘pace maker cells’ • Discharges rhythmically & responsible for initiation of rhythmic respiration • Located between nucleus ambiguus & lateral reticular formation on either side of the medulla • DRG & VRG respiratory neurons project to pre-BÖTC • It sends rhythmic impulses to phrenic motor neurons
Ventral group neurons (VRG) or Expiratory neurons • Located about 5mm anterior & lateral to DRG • It is a long column of neurons extends through the nucleus ambiguus & retro ambiguus in the ventro-lateral medulla • The long column of neurons has got rostral & caudal ‘E’ neurons, middle ‘I’ neurons • They are stimulated by impulses from DRG • They in turn inhibit DRG • In normal quiet respiration, their peripheral output are almost inactive • When sufficiently stimulated by higher respiratory drive (ventilation greater than normal), they stimulate expiratory muscles.
Pontine respiratory centers • Control the medullary respiratory centers activity • Two types • (Upper) Pneumotaxic center • (Lower) Apneustic center
Apneustic center • Present in lower pons – at the level of striae acusticae • Send stimulatory impulses to – DRG thereby prevent “switch off” the ramp signal –cause prolonged depth of respiration (Apneusis) & also Pneumotaxic center • Receive impulses from – • DRG –which is stimulatory & • Pneumotaxic center –which is inhibitory • Also from periphery (lungs) through vagus –which also is inhibitory
Pneumotaxic center • Located in the upper pontine region of (medial) nucleus parabrachialis & Kolliker-Fuse nuclei of the dorso-lateral pons • These neurons are stimulated by Apneustic center • In turn, they inhibit Apneustic center (when sufficiently stimulated). • Significance – • control of normal rhythmic respiration by sending impulses to apneustic center -- • With weak signal increase respiratory rate • With strong signal decrease respiratory rate • Damage of this area –respiration becomes slower & deeper (tidal volume is increased)
Section at various level of brain stem • A — Above pons (both respiratory centers are intact)– normal respiration • B – Mid pons (Pneumotaxic center of pons is removed)– Normal respiration –with intact vagus; Apneustic type of breathingwithout vagus • C – Between pons & medulla (only medullary center is present)– Air hunger breathing (shallow rapid breathing) • D – Below medulla (medullary center also removed) – Respiration ceases
Concept of production of Rhythmic respiratory cycle • Recent view: The rhythmic respiration is initiated by Pre-BÖtzinger complex, which has got pace maker cells which discharge rhythmically & send impulses to DRG. • The DRG neurons of medulla by firing ramp signal spontaneously (old concept) send these impulses to phrenic nerve to external inter-costal muscle bring about inspiration by producing slow & steady increase in lung volumes. • At the same time DRG stimulates both apneustic neurons & VRG neurons • This DRG ramp signals are strengthened by apneustic center activity. • Apneustic center also stimulate pnemotaxic center
Once pneumotaxic center is sufficiently stimulated; it in turn inhibits apneustic center. [In higher lung volumes (of > 1liter), the apneustic center can be inhibited through vagus (Herring-Brewer reflex)] Once apneustic center is inhibited, its drive on inspiratory center is stopped. Now with expiratory center (VRG) activity; the DRG neurons are inhibited which brought about abrupt stop of ramp signals. Expiration follows passively Next cycle repeats by producing ramp signal by DRG (initiated by Pre-BÖTC) In this, the respiratory rhythm is modified by both nervous (reflex) & chemical regulations [peripheral regulation of respiration].
Nervous regulation of respirationorReflex regulation of respirationor Non-chemical regulation of respiration
Types of nervous regulation of respiration • From respiratory tract through vagal afferents from receptors in the airways & lungs • Afferent from baroreceptors (arterial, atrial, ventricular & pulmonary) • Afferents from higher centers (cerebral, hypothalamus & limbic system) • Afferents from periphery through proprioceptors & visceral receptors • Effect of sleep on respiration
Role of vagal afferents from receptors in airways & lungs • Afferent fibers passing through the vagus nerve are – • Aortic nerve from aortic arch of baroreceptor & aortic body of chemoreceptor • Myelenated A δ fibers from airways – from a. Slow adapting stretch receptor; b. Rapid adapting stretch receptor; C. Irritant receptors • Non-myelenated C-fibers from lungs – from. ‘J’ receptor of alveoli & bronchi
Reflexes brought through vagal afferents • Hering-Breuer reflexes • Head’s paradoxical reflex • Reflexes through irritant receptors • ‘J’ receptor reflex
Hering-Breuer reflexes • I. Hering-Breuer inflation reflex – Inflation of lung (with higher volume >1liter) causes reflex arrest of inspiration & expiration starts. • Mechanism – • Stimulus – stretching of alveoli due to lung inflation • Stretch receptor (slow adapting receptor) –present in the alveoli • Afferent – through myelenated A δ fibers • Center –Apneustic center & Inspiratory center (DRG) –inhibitionon both • Effect – Inspiration stops & expiration starts passively • Significance – previously, it was considered, the normal rhythmic respiration is brought about by this reflex. Now it is proved, that this reflex acts only at higher volumes; hence helps to limit respiration in higher volumes (as in the case of exercise etc).
II. Hering-Breuer deflation reflex – If the lungs are deflated forcefully, inspiration starts Stimulus – forceful deflation of lungs Receptor – Rapid adapting receptor (lung irritant receptor) Afferent -- through myelenated A δ fibers Center –Inspiratory center (DRG) Effect -- stimulation
Head’s paradoxical reflex (After warming the vagi), when the lungs are inflated, instead of inhibition, inspiration is stimulated. • Indicating -- Presence of ‘positive feed back’ by separate group of nerve fibers
Reflexes through irritant receptors (rapid adapting receptors) • Located in air ways • Stimulus – • Inhalation of chemical & mechanical irritant gases & aerosols (ammonia & ether), cigarette smoke & carbon dust • Contraction of air way smooth muscle (by histamine or aerosols) • Collapse of alveoli (which pulls air ways)– due to pneumothorax, pulmonary congestion • (The following reflexes are elucidated)
1. Cough reflex –protective reflex; cough is a sudden forcible expiratory act. Stimulation of irritant receptors present in epiglottis, larynx, trachea by chemical & mechanical irritants. Afferent – Vagal A δ fibers Effect --Cough begins with a deep inspiration followed by forced expiration against closed glottis (intra pleural pressure goes up to >100 mm Hg) With sudden opening of glottis producing explosive outflow of air at velocities up to 1000 km/hr (3 to 4 times of PEFR) 2. Sneezing reflex –similar expiratory effort with continuously open glottis Significance of these two reflexes – help expel irritants & keep air ways clear
Juxta pulmonary-capillary receptorsorJuxta capillary receptorsor‘J’ receptors • Present in lung parenchyma close to capillary endothelium (Dawes, Mott & Widdicome in 1951) • Innervated by unmyelenated ‘C’ fibers (Paintal in 1958) • Stimulated by hyperinflation of the lungs & also by pulmonary edema • Effect – Apnoea followed by rapid shallow breathing & also bradycarida & hypotension & also inhibit spinal stretch reflex (limit exercise) • {also has chemo receptor effect – injection of capsaicin, nicotine, 5-hydorxythryptamine, phenyl biguanide stimulate these receptors and elucidate the same effect}
Afferent from baroreceptor • Located in carotid sinuses, aortic arch, (aslo in atria & ventricles) • Afferent –Sino-aortic nerves (buffer nerves) • Center –Respiratory center, Vasomotor center & Cardio-inhibitory center of medulla • Effect – Inhibition of respiration, vasodilation & decrease of Heart rate
Yawning –is a peculiar ‘infectious’ respiratory act –of deep inspiration followed by prolonged expiration. Physiological basis not known. However, under ventilated alveoli tend to collapse, by yawing (deep inspiration), the alveoli is stretched & open thereby prevent development of atelectasis. Yawning also increase venous return May be primitive ‘nonverbal signal’ for communication in animals Sighing – also have similar function
Afferent from propioceptors of muscles, tendons & joints (goes through dorsal column tract) – excite respiratory center Afferent from visceral receptors – Swallowing, vomiting & gagging –reflexly inhibit respiration Voluntary & involuntary abdominal muscles cause inhibition of respiration Hiccup –is spasmodic contraction of diaphragm that produces an inspiration during which the glottis suddenly closes. (Closure of glottis responsible for characteristic sensation & sound)
Role of sleep in respiration • Respiration is less rigorously controlled during sleep; because, • During sleep – • CO2 sensitive to respiratory drive is decreased, • stimuli from various proprioceptors are reduced • Sleep-apnea syndrome – • occur at any age • Symptoms – morning headache, fatigue, in extreme case lead to respiratory failure with normal lungs). • Patients are polycythemic, hypoxemic, hypercapnic • Cause – failure during sleep of the genioglossus muscles to contract during inspiration, resulting the tongue falls back & obstruct air way. • Apneic spells are common in premature infants • Sudden infant death syndrome (SIDS) –form of sleep apnea & apparently healthy infants are found dead in sleep.
Role of Higher centers in respiration • Stimulation of motor cortex –acceleration of respiration • Stimulation of medial surface of anterior cingulate gyrus & ventral surface of orbito-insulo-temporal polar cortex –inhibition of respiration • Limbic system (emotions) & • Hypothalamus (pain) –affect respiration • Voluntary control – from neocortex – to motor cortex to respiratory muscles via pyramidal tract
Ondine’s curse • Loss of automatic control without loss of voluntary control • Disease due to bulbar poliomyelitis or disease process that compress medulla, inadvertent surgical cut during antero-lateral cordotomy for releving pain • Ondine –in German legend, was a unfaithful mortal lover of a water nymph. The king of water nymph by curse took away all his autonomic function.